

Osimertinib in Japanese patients with EGFR T790M mutation-positive advanced non-small-cell lung cancer: AURA3 trial
- PMID: 29697876
- PMCID: PMC5989837
- DOI: 10.1111/cas.13623
Osimertinib in Japanese patients with EGFR T790M mutation-positive advanced non-small-cell lung cancer: AURA3 trial
Abstract
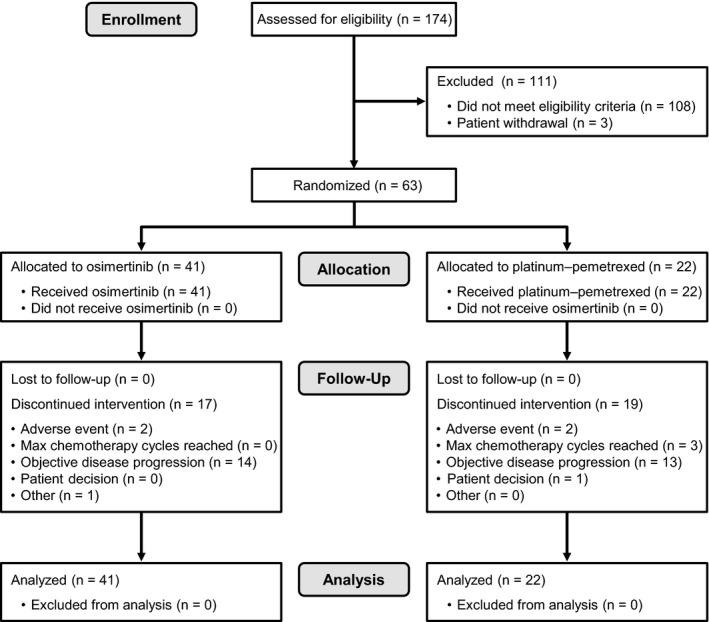
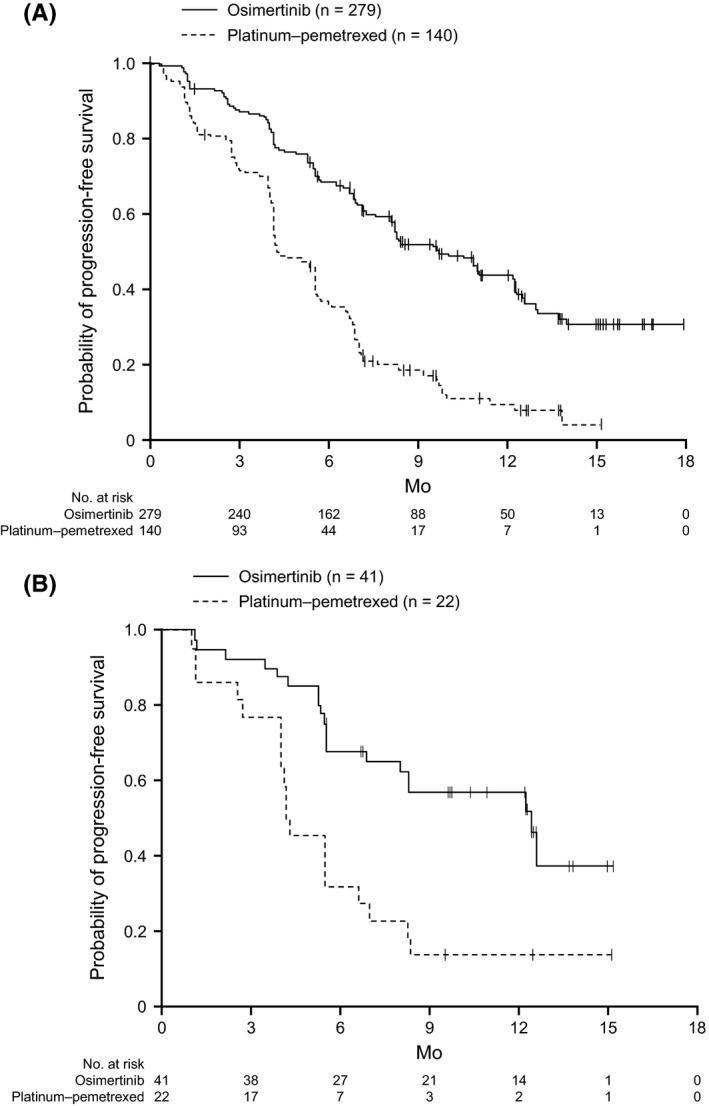
Epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) are the first-line treatment for patients with EGFR mutant non-small-cell lung cancer (NSCLC). However, most patients become resistant to these drugs, so their disease progresses. Osimertinib, a third-generation EGFR-TKI that can inhibit the kinase even when the common resistance-conferring Thr790Met (T790M) mutation is present, is a promising therapeutic option for patients whose disease has progressed after first-line EGFR-TKI treatment. AURA3 was a randomized (2:1), open-label, phase III study comparing the efficacy of osimertinib (80 mg/d) with platinum-based therapy plus pemetrexed (500 mg/m2 ) in 419 patients with advanced NSCLC with the EGFR T790M mutation in whom disease had progressed after first-line EGFR-TKI treatment. This subanalysis evaluated the safety and efficacy of osimertinib specifically in 63 Japanese patients enrolled in AURA3. The primary end-point was progression-free survival (PFS) based on investigator assessment. Improvement in PFS was clinically meaningful in the osimertinib group (n = 41) vs the platinum-pemetrexed group (n = 22; hazard ratio 0.27; 95% confidence interval, 0.13-0.56). The median PFS was 12.5 and 4.3 months in the osimertinib and platinum-pemetrexed groups, respectively. Grade ≥3 adverse events determined to be related to treatment occurred in 5 patients (12.2%) treated with osimertinib and 12 patients (54.5%) treated with platinum-pemetrexed. The safety and efficacy results in this subanalysis are consistent with the results of the overall AURA3 study, and support the use of osimertinib in Japanese patients with EGFR T790M mutation-positive NSCLC whose disease has progressed following first-line EGFR-TKI treatment. (ClinicalTrials.gov trial registration no. NCT02151981.).
Keywords: Japanese; epidermal growth factor receptor; mutation; non-small-cell lung cancer; tyrosine kinase.
© 2018 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Figures
References
-
- Tan DS, Yom SS, Tsao MS, et al. The International Association for the Study of Lung Cancer Consensus Statement on Optimizing Management of EGFR Mutation‐Positive Non‐Small Cell Lung Cancer: Status in 2016. J Thorac Oncol. 2016;11:946‐963. - PubMed
-
- Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non–small‐cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380‐2388. - PubMed
-
- Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non‐small‐cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11:121‐128. - PubMed
-
- Kobayashi S, Boggon TJ, Dayaram T, et al. EGFR mutation and resistance of non–small‐cell lung cancer to gefitinib. N Engl J Med. 2005;352:786‐792. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
