

National implementation of multi-parametric magnetic resonance imaging for prostate cancer detection - recommendations from a UK consensus meeting
- PMID: 29699001
- PMCID: PMC6334741
- DOI: 10.1111/bju.14361
National implementation of multi-parametric magnetic resonance imaging for prostate cancer detection - recommendations from a UK consensus meeting
Abstract
Objectives: To identify areas of agreement and disagreement in the implementation of multi-parametric magnetic resonance imaging (mpMRI) of the prostate in the diagnostic pathway.
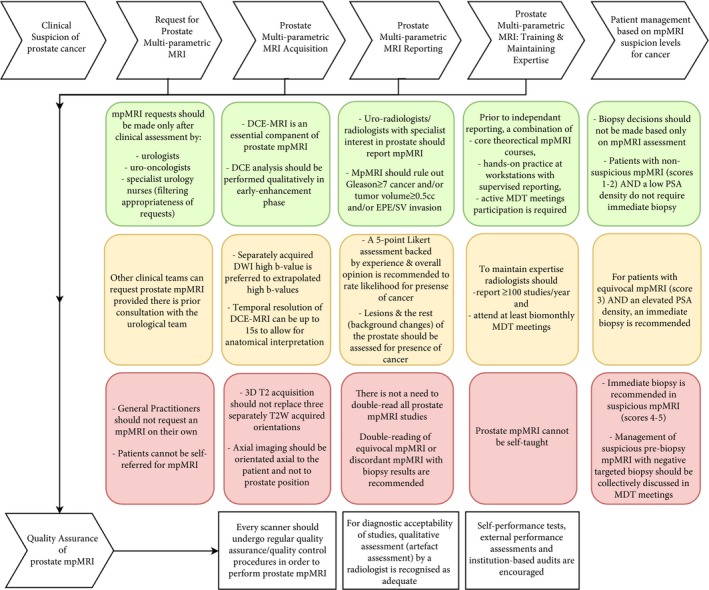
Materials and methods: Fifteen UK experts in prostate mpMRI and/or prostate cancer management across the UK (involving nine NHS centres to provide for geographical spread) participated in a consensus meeting following the Research and Development Corporation and University of California-Los Angeles (UCLA-RAND) Appropriateness Method, and were moderated by an independent chair. The experts considered 354 items pertaining to who can request an mpMRI, prostate mpMRI protocol, reporting guidelines, training, quality assurance (QA) and patient management based on mpMRI levels of suspicion for cancer. Each item was rated for agreement on a 9-point scale. A panel median score of ≥7 constituted 'agreement' for an item; for an item to reach 'consensus', a panel majority scoring was required.
Results: Consensus was reached on 59% of items (208/354); these were used to provide recommendations for the implementation of prostate mpMRI in the UK. Key findings include prostate mpMRI requests should be made in consultation with the urological team; mpMRI scanners should undergo QA checks to guarantee consistently high diagnostic quality scans; scans should only be reported by trained and experienced radiologists to ensure that men with unsuspicious prostate mpMRI might consider avoiding an immediate biopsy.
Conclusions: Our consensus statements demonstrate a set of criteria that are required for the practical dissemination of consistently high-quality prostate mpMRI as a diagnostic test before biopsy in men at risk.
Keywords: consensus methods; multi-parametric MRI; prostate cancer; recommendations.
© 2018 The Authors BJU International published by John Wiley & Sons Ltd on behalf of BJU International.
Figures
References
-
- Fütterer JJ, Briganti A, De Visschere P et al. Can clinically significant prostate cancer be detected with multiparametric magnetic resonance imaging? A systematic review of the literature. Eur Urol 2015; 68: 1045–53 - PubMed
-
- Schoots IG, Petrides N, Giganti F et al. Magnetic resonance imaging in active surveillance of prostate cancer: a systematic review. Eur Urol 2015; 67: 627–36 - PubMed
-
- National Institute for Health and Care Excellence . Prostate Cancer: Diagnosis and Management, Clinical Guideline [CG175], 2014. Available at: http://www.nice.org.uk/guidance/cg175/chapter/1-recommendations. Accessed April 2018
-
- Dickinson L, Ahmed HU, Hindley RG et al. Prostate‐specific antigen vs. magnetic resonance imaging parameters for assessing oncological outcomes after high intensity‐focused ultrasound focal therapy for localized prostate cancer. Urol Oncol 2017; 35: 30.e9–e15 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
