

Gonadotropin stimulation: past, present and future
- PMID: 29699102
- PMCID: PMC5906949
- DOI: 10.1007/s12522-011-0097-2
Gonadotropin stimulation: past, present and future
Abstract
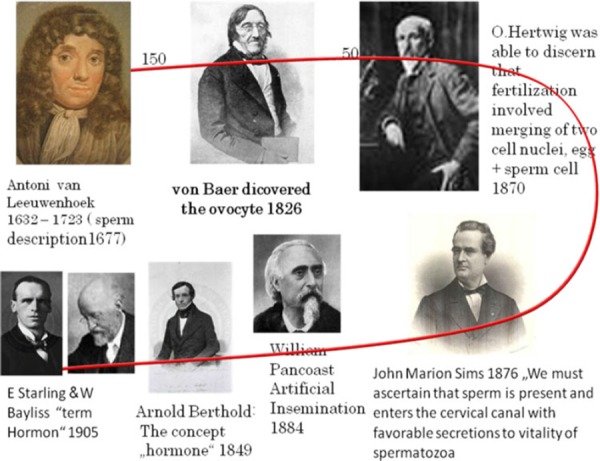
Gonadotropin therapy is so central to infertility treatment that it is easy to overlook the considerable discovery and research that preceded production of the effective and safe products available today. The history underpinning this development spans over 300 years and provides a splendid example of how basic animal experimentation and technological advances have progressed to clinical application. Following the discovery of germ cells in 1677 and realizing, in 1870, that fertilization involved the merging of two cell nuclei, one from the egg and one from sperm, it took another 40 years to discover the interplay between hypothalamus, pituitary and gonads. The potential roles of gonadotropin regulation were discovered in 1927. Gonadotropin, such as pregnant mare serum gonadotropin (PMSG), was first introduced for ovarian stimulation in 1930. However, use of PMSG leads to antibody formation, and had to be withdrawn. Following withdrawal of PMSG, human pituitary gonadotropin (HPG) and urinary menopausal gonadotropin (hMG) appeared on the market, and 50 years ago the first child was delivered by our group in 1961 and opened the path to controlled ovarian stimulation. HPG produced good results, but its use came to an end in the late 1980s when it was linked to the development of Creutzfeldt-Jakob disease (CJD). HMG preparations containing a high percentage of unknown urinary proteins, making quality control almost impossible, were then the only gonadotropins remaining on the market. With the availability of hMG, clomiphene citrate, ergot derivatives, GnRH agonists and antagonists, as well as metformin, algorithms were developed for their optimal utilization and were used for the next four decades. Following the first human IVF baby in 1978 and ICSI in 1991, such procedures became standard practice. The main agents for controlled ovarian stimulation for IVF were gonadotropins and GnRH analogues, with batch to batch consistent gonadotropic preparations; methods could be developed to predict and select the correct dose and the optimal protocol for each patient. We are now seeing the appearance of gonadotropin with sustained action and orally active GnRH analogues as well as orally active molecules capable to stimulate follicle growth and inducing ovulation. These new developments may one day remove the need for the classical gonadotropin in clinical work.
Keywords: FSH; Gonadotropins; Human reproduction; Infertility; LH.
Figures
References
-
- Vesalius, A. De humani corporis fabrica libri septem . Basileae [Basel]: Ex officina Joannis Oporini; 1543.
-
- Fallopius, G. Observationes anatomicae, Venise; 1561.
-
- De Graaf, R. De Mullerium Organis. Paris; 1672.
-
- Sims HM Sterility and the value of microscope in its diagnosis and treatment, vol 13, 1888. Boston: Trans Am Gynecol Soc;
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous