

In-flight angina pectoris; an unusual presentation
- PMID: 29699500
- PMCID: PMC5921980
- DOI: 10.1186/s12872-018-0797-1
In-flight angina pectoris; an unusual presentation
Abstract
Background: An unusual case of typical angina which occurred on a long haul flight is presented. This case is notable as this was the index presentation, with no previous symptoms prior to this. Physiological changes at altitude can be marked, and include hypoxia, tachycardia and an increase in cardiac output. These changes were enough to expose underlying angina in our patient.
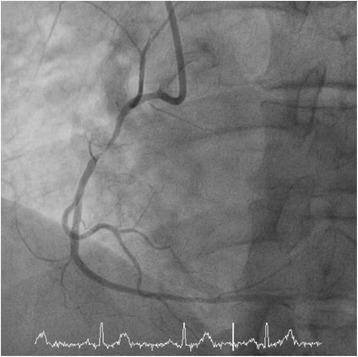
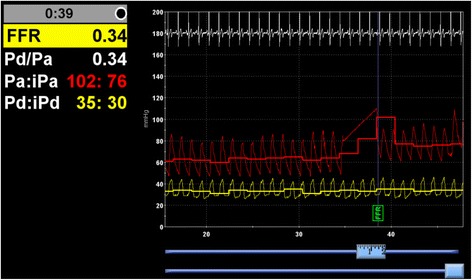
Case presentation: A 68 year old man presented with typical cardiac chest pain on a long haul flight. His symptoms first started 10-15 min after take-off and resolved on landing. This was his index presentation, and there were no similar symptoms in the past. Background history included hypercholesterolaemia and benign prostatic hypertrophy only. He led a rather sedentary lifestyle. A CT coronary angiogram showed significant disease in the proximal left anterior descending artery and proximal right coronary artery. He went on to have a coronary angiogram with invasive physiological measurements, which determined both lesions were physiologically significant. Both arteries were treated with drug eluting stents. Since treatment, he once again embarked on a long haul flight, and was completely asymptomatic.
Conclusion: The presentation of symptoms in this individual was rather unusual, but clearly caused by significant coronary artery disease. Potentially his sedentary lifestyle was not enough in day-to-day activities to promote anginal symptoms. When his cardiovascular system was physiologically stressed during flight, brought about by hypoxia, raised sympathetic tone and increased cardiac output, symptoms emerged. In turn, when landing, with atmospheric conditions normalised, physiological stress was removed, and symptoms resolved. Clinically therefore, one should not exclude symptoms that occur with differing physiological states, such as stress and altitude, as they are also potential triggers for myocardial ischaemia, despite absence of day-to-day symptoms.
Keywords: Angina; Coronary artery disease; Flight; Fractional flow reserve; Pressure wire.
Conflict of interest statement
Ethics approval and consent to participate
Procedures conducted were part of standard medical practice, and hence no formal ethical approval was sought.
Consent for publication
Full consent was obtained in written form from the patient for publication of relevant data, images, and medical history.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Fractional flow reserve for the assessment of complex multivessel disease in a patient after hybrid coronary revascularization.Catheter Cardiovasc Interv. 2013 Jun 1;81(7):1169-73. doi: 10.1002/ccd.24605. Epub 2013 Jan 23. Catheter Cardiovasc Interv. 2013. PMID: 22899601
-
Application of fractional flow reserve and optical coherence tomography examinations in a patient presenting with recurrent angina: a case report.J Med Case Rep. 2015 Aug 27;9:182. doi: 10.1186/s13256-015-0664-y. J Med Case Rep. 2015. PMID: 26307058 Free PMC article.
-
Type 4 dual left anterior descending coronary artery.Korean J Intern Med. 2015 Sep;30(5):727-9. doi: 10.3904/kjim.2015.30.5.727. Epub 2015 Aug 27. Korean J Intern Med. 2015. PMID: 26354068 Free PMC article. No abstract available.
-
API expert consensus document on management of ischemic heart disease.J Assoc Physicians India. 2006 Jun;54:469-80. J Assoc Physicians India. 2006. PMID: 16909697 Review.
-
Clinical Application of Fractional Flow Reserve-Guided Percutaneous Coronary Intervention for Stable Coronary Artery Disease.Curr Cardiol Rep. 2016 Apr;18(4):32. doi: 10.1007/s11886-016-0711-3. Curr Cardiol Rep. 2016. PMID: 26915010 Review.
Cited by
-
Chest compression quality decreases in hypoxic conditions simulating an airliner cabin at cruising altitude: a randomized, controlled, double-blind Manikin Study.Sci Rep. 2024 Oct 29;14(1):25971. doi: 10.1038/s41598-024-77149-4. Sci Rep. 2024. PMID: 39472462 Free PMC article. Clinical Trial.
-
Acupuncture on treating angina pectoris: A systematic review.Medicine (Baltimore). 2020 Jan;99(2):e18548. doi: 10.1097/MD.0000000000018548. Medicine (Baltimore). 2020. PMID: 31914030 Free PMC article.
References
-
- Chest pain of recent onset: assessment and diagnosis. (NICE Guideline CG95). National Institute for Health and Care Excellence (2010, Updated 2016). https://www.nice.org.uk/guidance/cg95. Accessed 20 Jan 2018. - PubMed
-
- Cottrell JJ. Altitude exposures during aircraft flight: flying higher. Chest. 1992;92:81–84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
