

Urinary biomarkers predict advanced acute kidney injury after cardiovascular surgery
- PMID: 29699579
- PMCID: PMC5921971
- DOI: 10.1186/s13054-018-2035-8
Urinary biomarkers predict advanced acute kidney injury after cardiovascular surgery
Abstract
Background: Acute kidney injury (AKI) after cardiovascular surgery is a serious complication. Little is known about the ability of novel biomarkers in combination with clinical risk scores for prediction of advanced AKI.
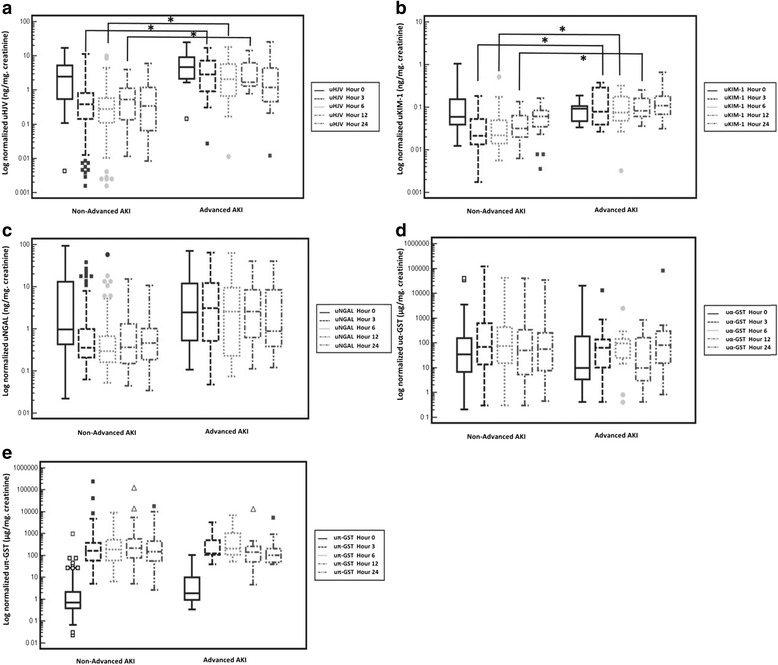
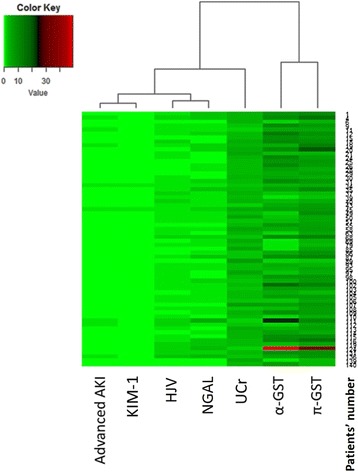
Methods: In this prospectively conducted multicenter study, urine samples were collected from 149 adults at 0, 3, 6, 12 and 24 h after cardiovascular surgery. We measured urinary hemojuvelin (uHJV), kidney injury molecule-1 (uKIM-1), neutrophil gelatinase-associated lipocalin (uNGAL), α-glutathione S-transferase (uα-GST) and π-glutathione S-transferase (uπ-GST). The primary outcome was advanced AKI, under the definition of Kidney Disease: Improving Global Outcomes (KDIGO) stage 2, 3 and composite outcomes were KDIGO stage 2, 3 or 90-day mortality after hospital discharge.
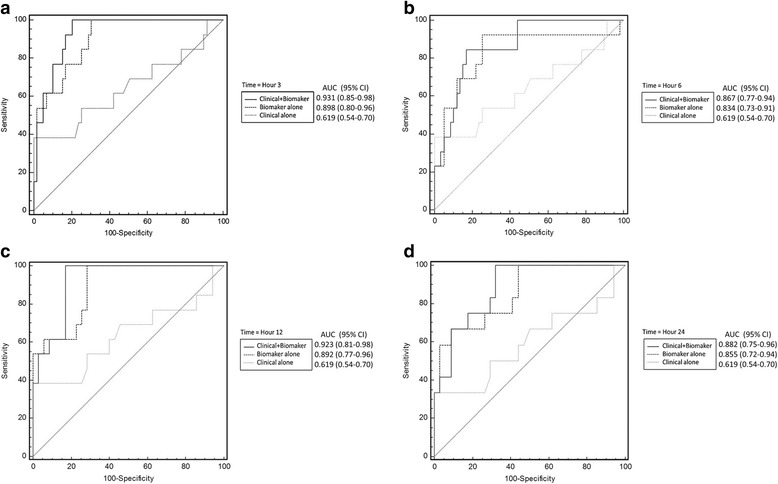
Results: Patients with advanced AKI had significantly higher levels of uHJV and uKIM-1 at 3, 6 and 12 h after surgery. When normalized by urinary creatinine level, uKIM-1 in combination with uHJV at 3 h post-surgery had a high predictive ability for advanced AKI and composite outcome (AUC = 0.898 and 0.905, respectively). The combination of this biomarker panel (normalized uKIM-1, uHJV at 3 h post-operation) and Liano's score was superior in predicting advanced AKI (AUC = 0.931, category-free net reclassification improvement of 1.149, and p < 0.001).
Conclusions: When added to Liano's score, normalized uHJV and uKIM-1 levels at 3 h after cardiovascular surgery enhanced the identification of patients at higher risk of progression to advanced AKI and composite outcomes.
Keywords: Acute kidney injury; Biomarkers; Hemojuvelin; Kidney injury molecule-1; Liano’s score; Neutrophil gelatinase-associated lipocalin; α-Glutathione S-transferase; π-Glutathione S-transferase.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the research ethics review board of National Taiwan University Hospital (201105040RC) along with established written informed consent. This research was carried out in accordance with the approved guidelines. Written informed consent was obtained from all participants before inclusion.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Zarbock A, Kellum JA, Schmidt C, Van Aken H, Wempe C, Pavenstadt H, Boanta A, Gerss J, Meersch M. Effect of early vs delayed initiation of renal replacement therapy on mortality in critically ill patients with acute kidney injury: the ELAIN randomized clinical trial. JAMA. 2016;315(20):2190–2199. doi: 10.1001/jama.2016.5828. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
