

Impact of a Primary Care CKD Registry in a US Public Safety-Net Health Care Delivery System: A Pragmatic Randomized Trial
- PMID: 29699885
- PMCID: PMC6057801
- DOI: 10.1053/j.ajkd.2018.01.058
Impact of a Primary Care CKD Registry in a US Public Safety-Net Health Care Delivery System: A Pragmatic Randomized Trial
Abstract
Background: Many individuals with chronic kidney disease (CKD) do not receive guideline-concordant care. We examined the impact of a team-based primary care CKD registry on clinical measures and processes of care among patients with CKD cared for in a public safety-net health care delivery system.
Study design: Pragmatic trial of a CKD registry versus a usual-care registry for 1 year.
Setting & participants: Primary care providers (PCPs) and their patients with CKD in a safety-net primary care setting in San Francisco.
Intervention: The CKD registry identified at point of care all patients with CKD, those with blood pressure (BP)>140/90mmHg, those without angiotensin-converting enzyme (ACE) inhibitor/angiotensin receptor blocker (ARB) prescription, and those without albuminuria quantification in the past year. It also provided quarterly feedback pertinent to these metrics to promote "outreach" to patients with CKD. The usual-care registry provided point-of-care cancer screening and immunization data.
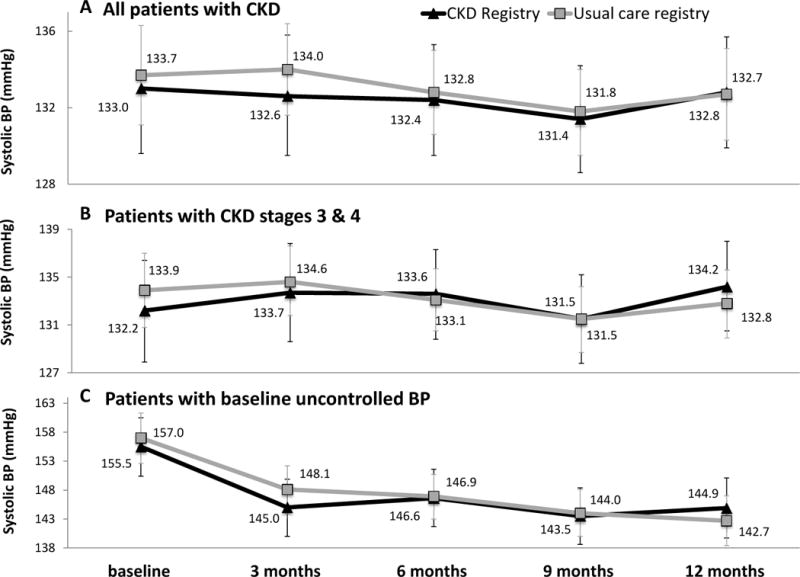
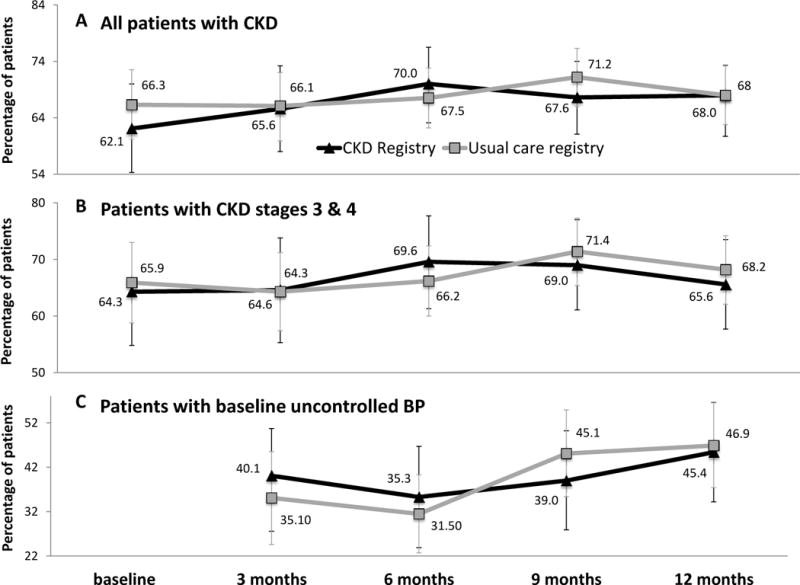
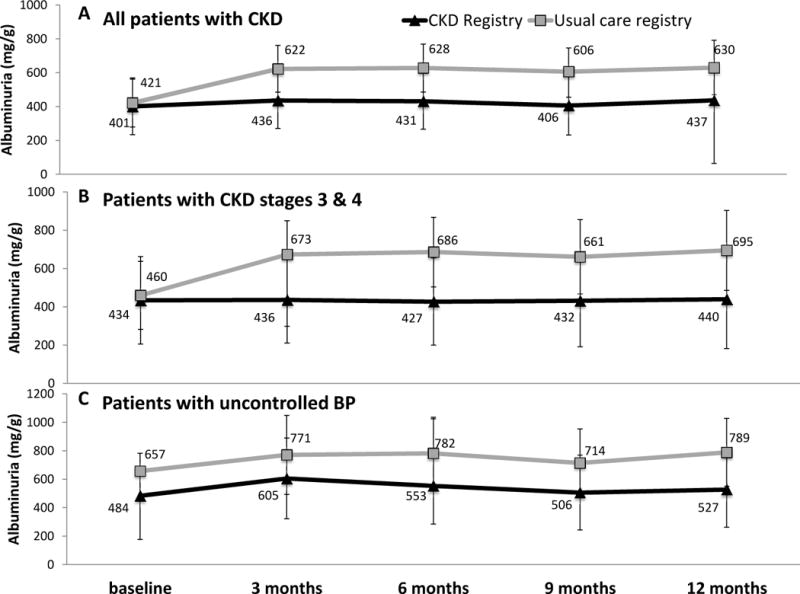
Outcomes: Changes in systolic BP at 12 months (primary outcome), proportion of patients with BP control, prescription of ACE inhibitors/ARBs, quantification of albuminuria, severity of albuminuria, and estimated glomerular filtration rate.
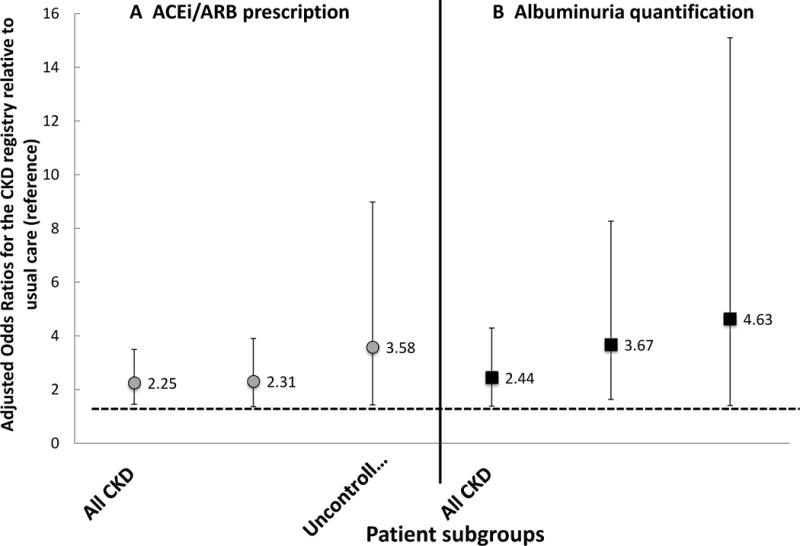
Results: The patient population (n=746) had a mean age of 56.7±12.1 (standard deviation) years, was 53% women, and was diverse (8% non-Hispanic white, 35.7% black, 24.5% Hispanic, and 24.4% Asian). Randomization to the CKD registry (30 PCPs, 285 patients) versus the usual-care registry (49 PCPs, 461 patients) was associated with 2-fold greater odds of ACE inhibitor/ARB prescription (adjusted OR, 2.25; 95% CI, 1.45-3.49) and albuminuria quantification (adjusted OR, 2.44; 95% CI, 1.38-4.29) during the 1-year study period. Randomization to the CKD registry was not associated with changes in systolic BP, proportion of patients with uncontrolled BP, or degree of albuminuria or estimated glomerular filtration rate.
Limitations: Potential misclassification of CKD; missing baseline medication data; limited to study of a public safety-net health care system.
Conclusions: A team-based safety-net primary care CKD registry did not improve BP parameters, but led to greater albuminuria quantification and more ACE inhibitor/ARB prescriptions after 1 year. Adoption of team-based CKD registries may represent an important step in translating evidence into practice for CKD management.
Keywords: CKD management; CKD registry; Chronic kidney disease (CKD); albuminuria; angiotensin converting enzyme inhibitors (ACEi); angiotensin receptor blockers (ARB); best practices; blood pressure control; disease progression; evidence-based care; guideline implementation; hypertension; pragmatic trial; process of care.
Copyright © 2018 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure: The authors declare that they have no relevant financial interests.
Figures
Comment in
-
Improving Primary Care for Patients With CKD in the Digital Era.Am J Kidney Dis. 2018 Aug;72(2):159-160. doi: 10.1053/j.ajkd.2018.03.016. Am J Kidney Dis. 2018. PMID: 30037473 No abstract available.
References
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–2047. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–1305. - PubMed
-
- Barrett BJ. Applying multiple interventions in chronic kidney disease. Semin Dial. 2003;16(2):157–164. - PubMed
-
- Sarnak MJ, Greene T, Wang X, et al. The effect of a lower target blood pressure on the progression of kidney disease: long-term follow-up of the modification of diet in renal disease study. Ann Intern Med. 2005;142(5):342–351. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
