

Lifetime risk of atrial fibrillation according to optimal, borderline, or elevated levels of risk factors: cohort study based on longitudinal data from the Framingham Heart Study
- PMID: 29699974
- PMCID: PMC5917175
- DOI: 10.1136/bmj.k1453
Lifetime risk of atrial fibrillation according to optimal, borderline, or elevated levels of risk factors: cohort study based on longitudinal data from the Framingham Heart Study
Abstract
Objective: To examine the association between risk factor burdens-categorized as optimal, borderline, or elevated-and the lifetime risk of atrial fibrillation.
Design: Community based cohort study.
Setting: Longitudinal data from the Framingham Heart Study.
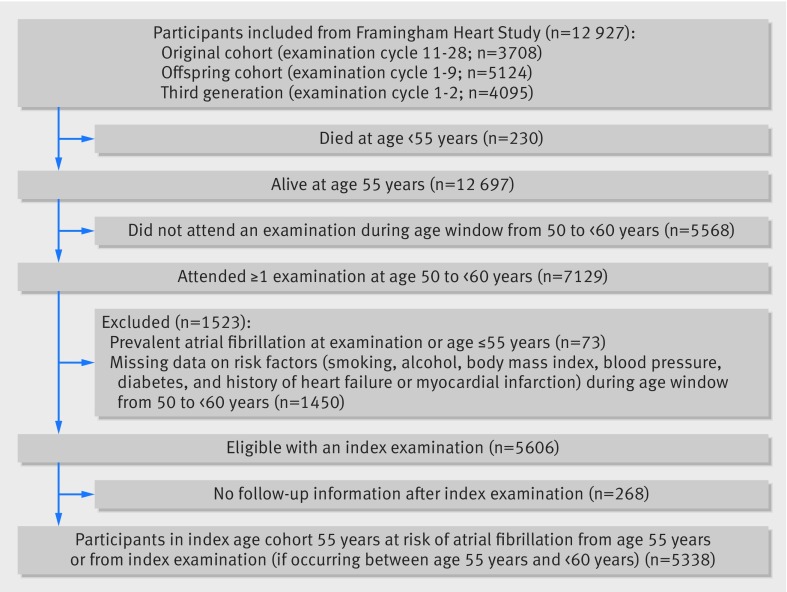
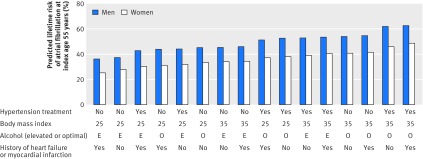
Participants: Individuals free of atrial fibrillation at index ages 55, 65, and 75 years were assessed. Smoking, alcohol consumption, body mass index, blood pressure, diabetes, and history of heart failure or myocardial infarction were assessed as being optimal (that is, all risk factors were optimal), borderline (presence of borderline risk factors and absence of any elevated risk factor), or elevated (presence of at least one elevated risk factor) at index age.
Main outcome measure: Lifetime risk of atrial fibrillation at index age up to 95 years, accounting for the competing risk of death.
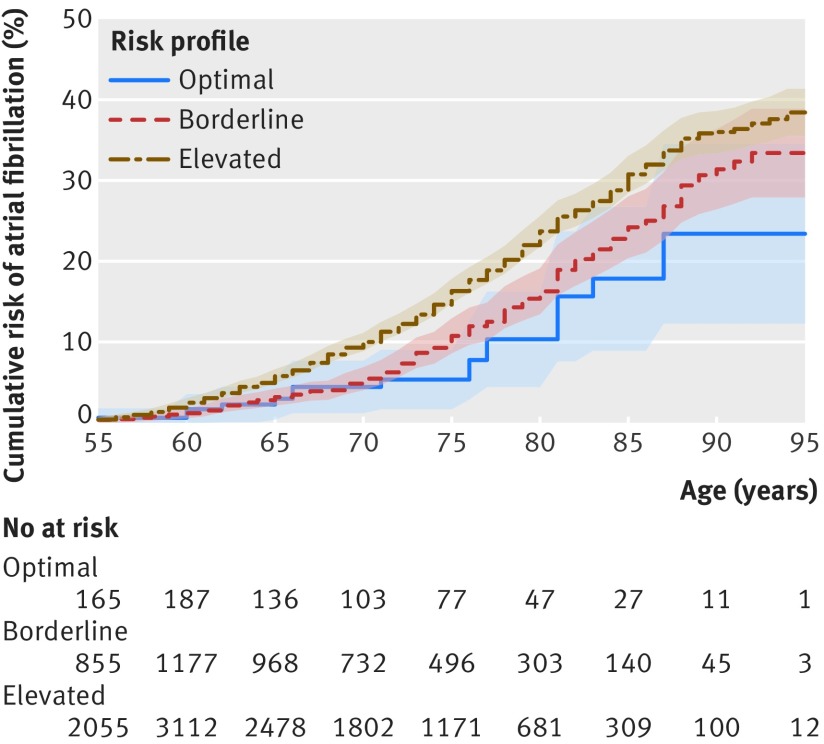
Results: At index age 55 years, the study sample comprised 5338 participants (2531 (47.4%) men). In this group, 247 (4.6%) had an optimal risk profile, 1415 (26.5%) had a borderline risk profile, and 3676 (68.9%) an elevated risk profile. The prevalence of elevated risk factors increased gradually when the index ages rose. For index age of 55 years, the lifetime risk of atrial fibrillation was 37.0% (95% confidence interval 34.3% to 39.6%). The lifetime risk of atrial fibrillation was 23.4% (12.8% to 34.5%) with an optimal risk profile, 33.4% (27.9% to 38.9%) with a borderline risk profile, and 38.4% (35.5% to 41.4%) with an elevated risk profile. Overall, participants with at least one elevated risk factor were associated with at least 37.8% lifetime risk of atrial fibrillation. The gradient in lifetime risk across risk factor burden was similar at index ages 65 and 75 years.
Conclusions: Regardless of index ages at 55, 65, or 75 years, an optimal risk factor profile was associated with a lifetime risk of atrial fibrillation of about one in five; this risk rose to more than one in three a third in individuals with at least one elevated risk factor.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: main support from the Boston University School of Medicine, and the National Heart, Lung, and Blood Institute’s Framingham Heart Study for the submitted work; SAL reports personal fees from St Jude Medical/Abbott and Quest Diagnostics, and grants from Boehringer Ingelheim, Biotronik, and Bayer HealthCare outside the submitted work; PTE reports grants from National Institutes of Health (NIH; K24HL105780), Established Investigator Award from the American Heart Association (13EIA14220013), Foundation Leducq (14CVD01), and Bayer HealthCare outside the submitted work; DDM receives sponsored research support from Bristol Myers Squibb, Pfizer, Biotronik, and Philips Healthcare, has consulted for Bristol Myers Squibb, FlexCon, Samsung, Philips, and Pfizer, has equity in Mobile Sense Technologies; and received grants from the NIH (R01HL126911, R01HL135219, R01HL136660, UH3 TR000921-04) and National Science Foundation (NSF-12-512) outside the submitted work; LF reports personal fees from Pfizer outside the submitted work; EJB reports funding from 1R01HL128914, 2R01 HL092577, 1P50HL120163, and the Robert Wood Johnson Foundation.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical