

Antibiotic Allergy in Pediatrics
- PMID: 29700201
- PMCID: PMC5914499
- DOI: 10.1542/peds.2017-2497
Antibiotic Allergy in Pediatrics
Abstract
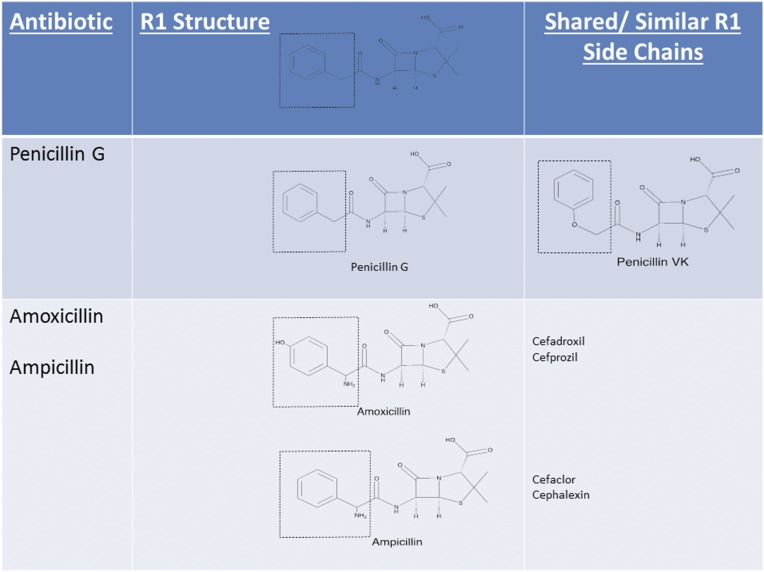
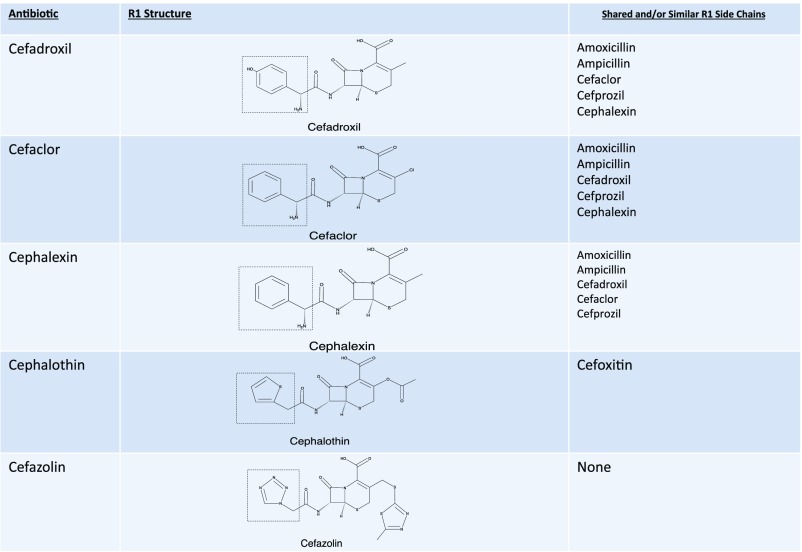
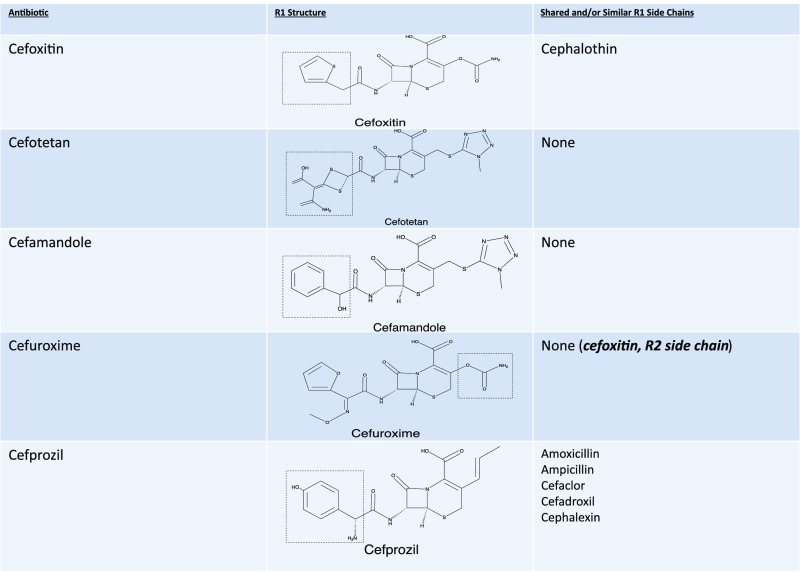
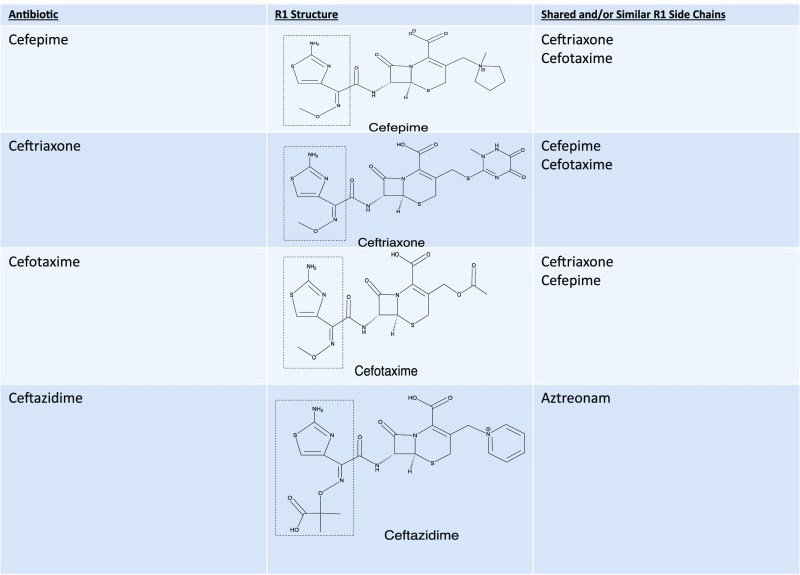
The overlabeling of pediatric antibiotic allergy represents a huge burden in society. Given that up to 10% of the US population is labeled as penicillin allergic, it can be estimated that at least 5 million children in this country are labeled with penicillin allergy. We now understand that most of the cutaneous symptoms that are interpreted as drug allergy are likely viral induced or due to a drug-virus interaction, and they usually do not represent a long-lasting, drug-specific, adaptive immune response to the antibiotic that a child received. Because most antibiotic allergy labels acquired in childhood are carried into adulthood, the overlabeling of antibiotic allergy is a liability that leads to unnecessary long-term health care risks, costs, and antibiotic resistance. Fortunately, awareness of this growing burden is increasing and leading to more emphasis on antibiotic allergy delabeling strategies in the adult population. There is growing literature that is used to support the safe and efficacious use of tools such as skin testing and drug challenge to evaluate and manage children with antibiotic allergy labels. In addition, there is an increasing understanding of antibiotic reactivity within classes and side-chain reactions. In summary, a better overall understanding of the current tools available for the diagnosis and management of adverse drug reactions is likely to change how pediatric primary care providers evaluate and treat patients with such diagnoses and prevent the unnecessary avoidance of antibiotics, particularly penicillins.
Copyright © 2018 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
References
-
- Vyles D, Chiu A, Simpson P, Nimmer M, Adams J, Brousseau DC. Parent-reported penicillin allergy symptoms in the pediatric emergency department. Acad Pediatr. 2017;17(3):251–255 - PubMed
-
- Chiriac AM; Demoly P . Drug Allergy. In: Leung DY, Sampson HA, Bonilla FA, Akdis CA, Szefler SJ, eds. Pediatric Allergy: Principles and Practice, 3rd ed . Edinburgh: Elsevier; 2016:498–504
-
- MacFadden DR, LaDelfa A, Leen J, et al. Impact of reported beta-lactam allergy on inpatient outcomes: a multicenter prospective cohort study. Clin Infect Dis. 2016;63(7):904–910 - PubMed
-
- Macy E, Contreras R. Health care use and serious infection prevalence associated with penicillin “allergy” in hospitalized patients: a cohort study. J Allergy Clin Immunol. 2014;133(3):790–796 - PubMed
-
- Vyles D, Adams J, Chiu A, Simpson P, Nimmer M, Brousseau DC. Allergy testing in children with low-risk penicillin allergy symptoms. Pediatrics. 2017;140(2):e20170471. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
