

Anesthesia Management of Modified Ex Vivo Liver Resection and Autotransplantation
- PMID: 29700275
- PMCID: PMC6248320
- DOI: 10.12659/AOT.907796
Anesthesia Management of Modified Ex Vivo Liver Resection and Autotransplantation
Abstract
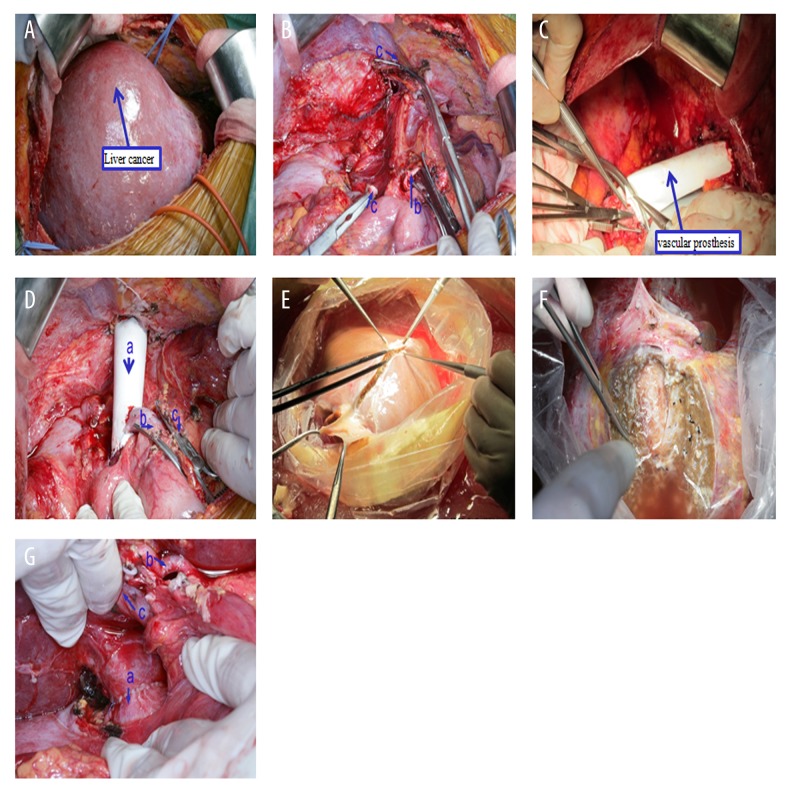
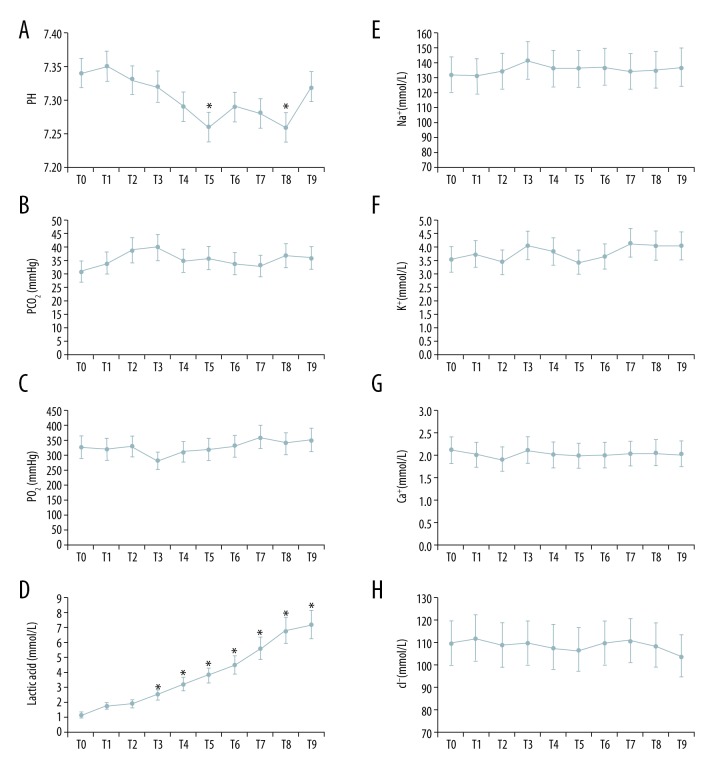
BACKGROUND Ex situ liver surgery allows liver resection and vascular reconstruction in patients who have liver tumors located in critical sites. Only a small series of studies about ex situ liver surgery is available in the literature. No anesthesia management experience has been previously published. The aim of the currents study was to summarize our experience with anesthetic management of patients during ex vivo liver surgery. MATERIAL AND METHODS The first 43 patients who received ex vivo liver surgery between January 2007 and April 2012 were included. A pulmonary artery catheter (PAC), transesophageal echocardiography (TEE), and pulse indicator continuous cardiac output (PiCCO) were used intraoperatively in the patients to monitor the hemodynamic changes. Thromboelastogram and the plasma coagulation test were used to monitor the coagulation changes. RESULTS All patients received general anesthesia with rapid sequence induction. The data obtained by PAC, TEE, and PiCOO in these cases showed large changes in hemodynamics during the stages of the first or second vessel reconstruction. The CI decreased about 59%/63% and the MPAP decreased about 49%/37% during the first/second vessel reconstruction. Accurate judgment of the dosage of active drug for vascular support is the key for the stabilization of hemodynamics as quickly as possible. However, a high incidence (35.5%) of prophase fibrinolysis in a long anhepatic phase should be monitored and managed. CONCLUSIONS Ex vivo liver surgery is no longer experimental and is a therapeutic option for patients with liver cancer in critical sites. Good anesthesia support is an essential element of liver autotransplantation.
Figures



References
-
- Jawan B, Wang CH, Chen CL, et al. Review of anesthesia in liver transplantation. Acta Anaesthesiol Taiwan. 2014;52(4):185–96. - PubMed
-
- Oldhafer KJ, Lang H, Schlitt HJ, et al. Long-term experience after ex situ liver surgery. Surgery. 2000;127(5):520–27. - PubMed
-
- Chui A. Ex situ ex vivo liver resection, partial liver autotransplantation for advanced hilar cholangiocarcinoma: A case report. Transplant Proc. 2003;35(1):402–3. - PubMed
-
- Vicente E, Quijano Y, Ielpo B, et al. Ex situ hepatectomy and liver autotransplantation for cholangiocarcinoma. Ann Surg Oncol. 2017;24(13):3990. - PubMed
-
- Baker MA, Maley WR, Needleman L, Doria C. Ex vivo resection of hepatic neoplasia and autotransplantation: A case report and review of the literature. J Gastrointest Surg. 2015;19(6):1169–76. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
