

Timing of elective pre-labour caesarean section: A decision analysis
- PMID: 29700811
- PMCID: PMC6492094
- DOI: 10.1111/ajo.12821
Timing of elective pre-labour caesarean section: A decision analysis
Abstract
Background: Since caesarean sections (CSs) before 39+0 weeks gestation are associated with higher rates of neonatal respiratory morbidity, it is recommended to delay elective CSs until 39+0 weeks. However, this bears the risk of earlier spontaneous labour resulting in unplanned CSs, which has workforce and resource implications, specifically in smaller obstetric units.
Aim: To assess, in a policy of elective CSs from 39+0 weeks onward, the number of unplanned CSs to prevent one neonate with respiratory complications, as compared to early elective CS.
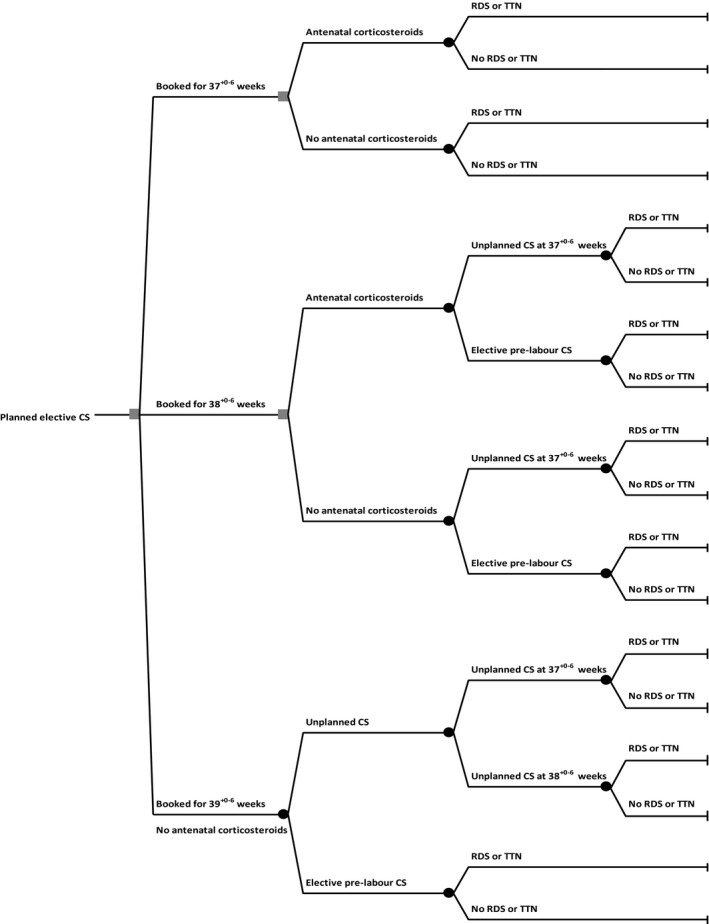
Materials and methods: We performed a decision analysis comparing early term elective CS at 37+0-6 or 38+0-6 weeks to elective prelabour CS, without strict medical indication, at 39+0-6 weeks, with earlier unplanned CS, in women with uncomplicated singleton pregnancies. We used literature data to calculate the number of unplanned CSs necessary to prevent one neonate with respiratory morbidity.
Results: Planning all elective CSs at 39+0-6 weeks required 10.9 unplanned CSs to prevent one neonate with respiratory morbidity, compared to planning all elective CSs at 38+0-6 weeks. Compared to planning all elective CSs at 37+0-6 weeks we needed to perform 3.3 unplanned CSs to prevent one neonate with respiratory morbidity.
Conclusion: In a policy of planning all elective pre-labour CSs from 39+0 weeks of gestation onward, between three and 11 unplanned CSs have to be performed to prevent one neonate with respiratory morbidity. Therefore, in our opinion, fear of early term labour and workforce disutility is no argument for scheduling elective CSs <39+0 weeks.
Keywords: caesarean section; decision analysis; neonatal respiratory morbidity; respiratory distress syndrome; transient tachypnoea of the newborn.
© 2018 The Authors. Australian and New Zealand Journal of Obstetrics and Gynaecology published by John Wiley & Sons Australia, Ltd on behalf of Royal Australian and New Zealand College of Obstetricians and Gynaecologists.
Figures
Comment in
-
Deliveries at early term gestation: A view from the NICU.Aust N Z J Obstet Gynaecol. 2019 Apr;59(2):E7. doi: 10.1111/ajo.12961. Aust N Z J Obstet Gynaecol. 2019. PMID: 30950046 No abstract available.
-
Re: Deliveries at early term gestation: A view from the NICU.Aust N Z J Obstet Gynaecol. 2019 Jun;59(3):E10. doi: 10.1111/ajo.12975. Aust N Z J Obstet Gynaecol. 2019. PMID: 31169318 No abstract available.
References
-
- Australian Institute of Health and Welfare . Australia's mothers and babies 2015 ‐ in brief. Perinatal statistics series no. 33. Cat. no. PER 91. Canberra: AIHW, 2017.
-
- Hilder L, Zhichao Z, Parker M et al Australia's mothers and babies 2012. Perinatal statistics series no. 30. Cat. no. PER 69. Canberra: AIHW, 2014.
-
- Levine EM, Ghai V, Barton JJ, Strom CM. Mode of delivery and risk of respiratory diseases in newborns. Obstet Gynecol 2001; 97: 439–442. - PubMed
-
- Kolas T, Saugstad OD, Daltveit AK et al Planned cesarean versus planned vaginal delivery at term: comparison of newborn infant outcomes. Am J Obstet Gynecol 2006; 195: 1538–1543. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
