

Measurement of Current Substance Use in a Cohort of HIV-Infected Persons in Continuity HIV Care, 2007-2015
- PMID: 29701832
- PMCID: PMC6118067
- DOI: 10.1093/aje/kwy092
Measurement of Current Substance Use in a Cohort of HIV-Infected Persons in Continuity HIV Care, 2007-2015
Abstract
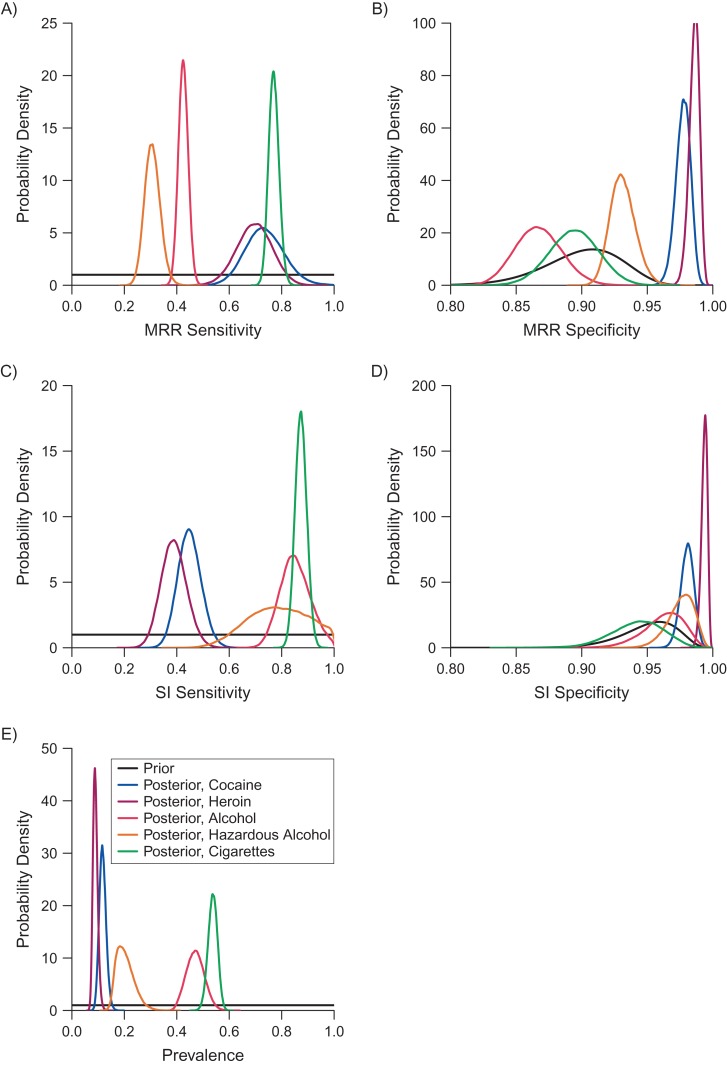
Accurate, routine measurement of recent illicit substance use is challenging. The Johns Hopkins Human Immunodeficiency Virus Clinical Cohort (Baltimore, Maryland) collects 2 imperfect but routine measurements of recent substance use: medical record review and self-interview. We used Bayesian latent class modeling to estimate sensitivity and specificity of each measurement as well as prevalence of substance use among 2,064 patients engaged in care during 2007-2015. Sensitivity of medical record review was higher than sensitivity of self-interview for cocaine and heroin use; posterior estimates ranged from 44% to 76% for cocaine use and from 39% to 67% for heroin use, depending on model assumptions and priors. In contrast, sensitivity of self-interview was higher than sensitivity of medical record review for any alcohol use, hazardous alcohol use, and cigarette smoking. Posterior estimates of sensitivity of self-interview were generally above 80%, 85%, and 87% for each substance, respectively. Specificity was high for all measurements. From one model, we estimated prevalence of substance use in the cohort to be 12.5% for cocaine, 9.3% for heroin, 48.5% for alcohol, 21.4% for hazardous alcohol, and 55.4% for cigarettes. Prevalence estimates from other models were generally comparable. Measurement error of substance use is nontrivial and should be accounted for in subsequent analyses.
Figures
References
-
- Lucas GM, Griswold M, Gebo KA, et al. . Illicit drug use and HIV-1 disease progression: a longitudinal study in the era of highly active antiretroviral therapy. Am J Epidemiol. 2006;163(5):412–420. - PubMed
-
- Poundstone KE, Chaisson RE, Moore RD. Differences in HIV disease progression by injection drug use and by sex in the era of highly active antiretroviral therapy. AIDS. 2001;15(9):1115–1123. - PubMed
-
- Moore RD, Keruly JC, Chaisson RE. Differences in HIV disease progression by injecting drug use in HIV-infected persons in care. J Acquir Immune Defic Syndr. 2004;35(1):46–51. - PubMed
-
- Baum MK, Rafie C, Lai S, et al. . Crack-cocaine use accelerates HIV disease progression in a cohort of HIV-positive drug users. J Acquir Immune Defic Syndr. 2009;50(1):93–99. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
