

The impact of direct-acting antiviral agents on liver and kidney transplant costs and outcomes
- PMID: 29701909
- PMCID: PMC6409105
- DOI: 10.1111/ajt.14895
The impact of direct-acting antiviral agents on liver and kidney transplant costs and outcomes
Abstract
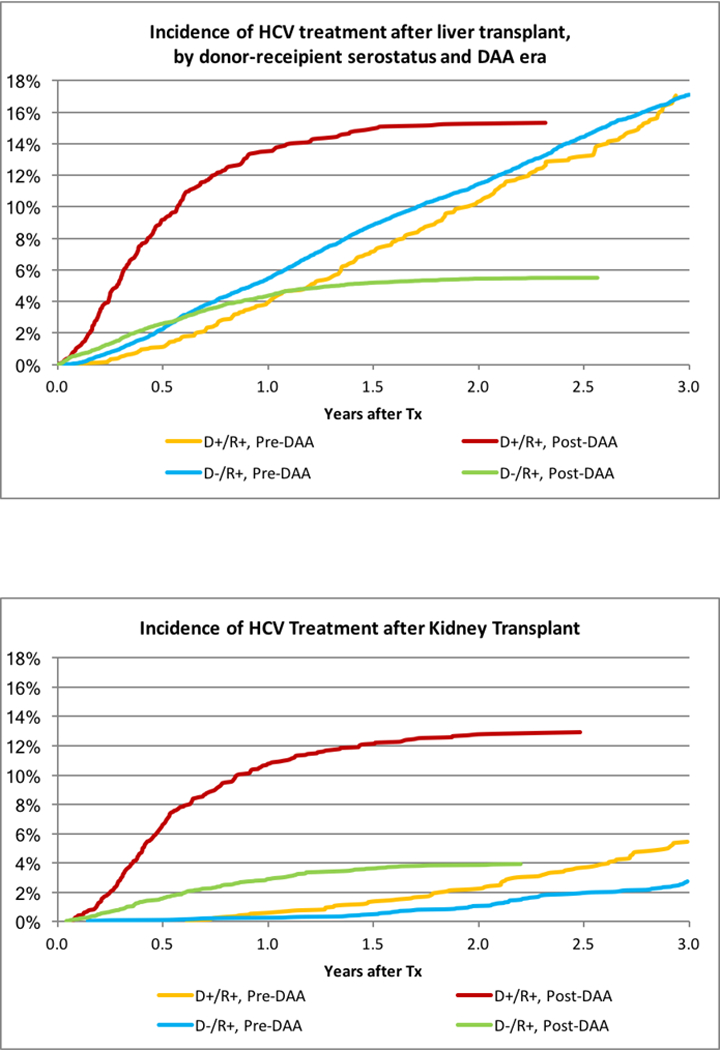
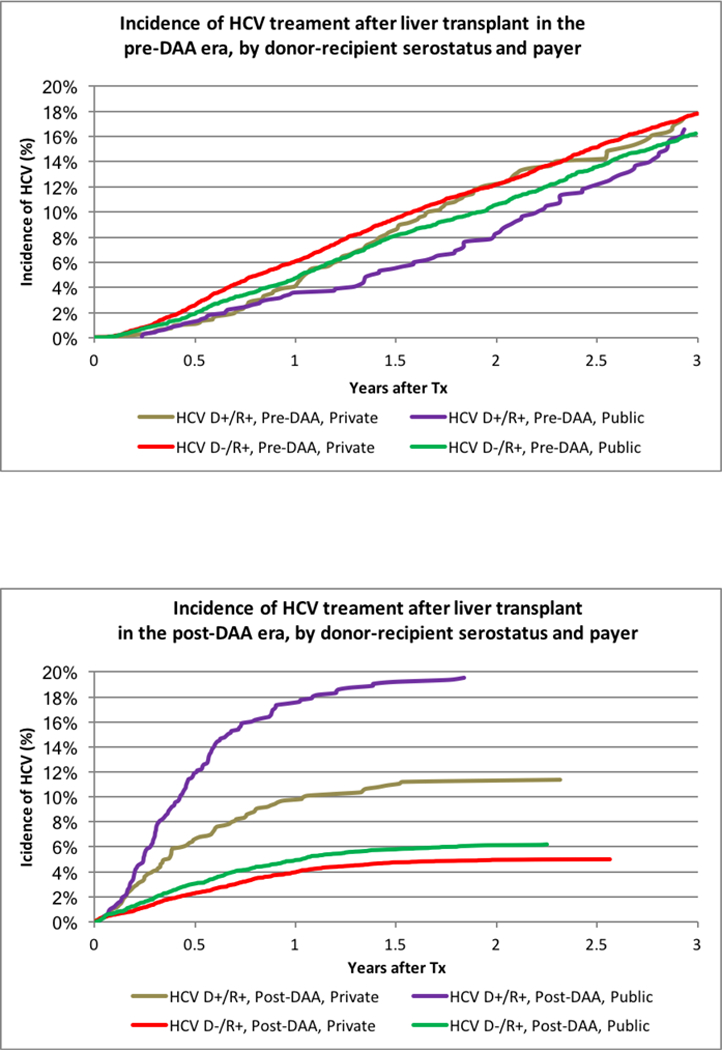
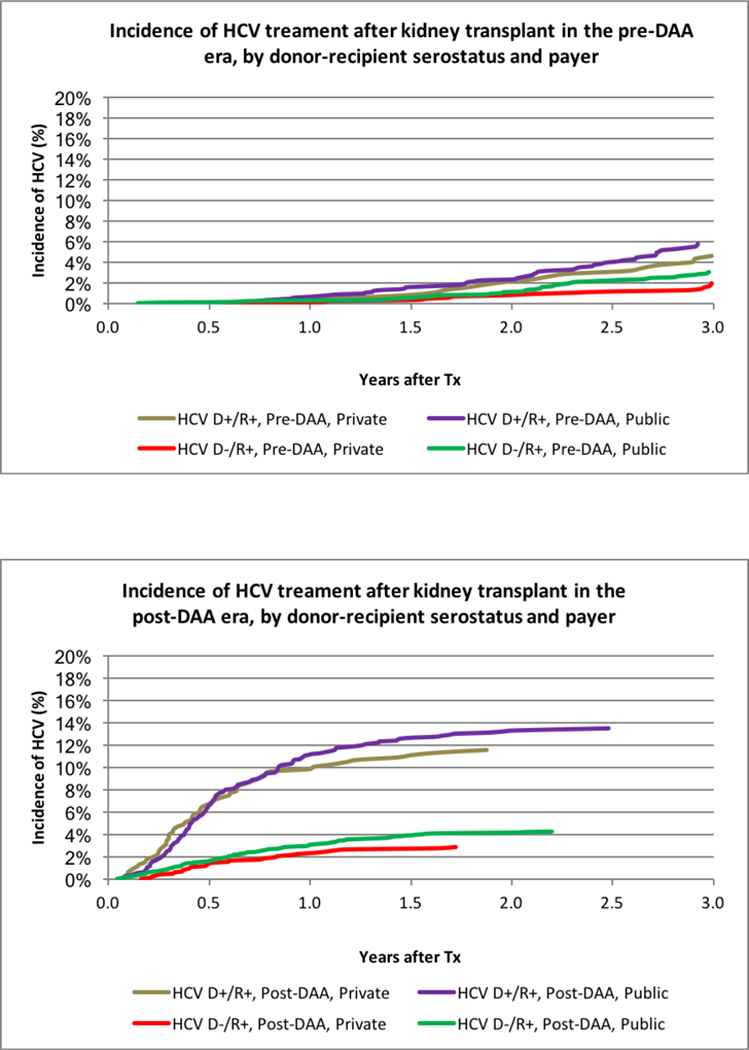
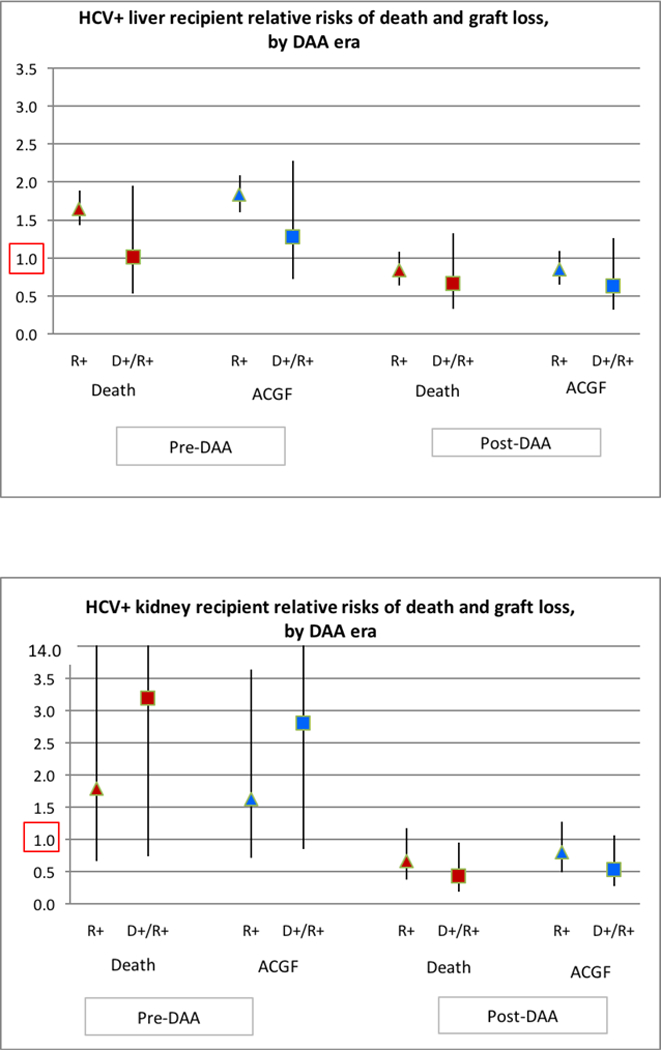
Direct-acting antiviral medications (DAAs) have revolutionized care for hepatitis C positive (HCV+) liver (LT) and kidney (KT) transplant recipients. Scientific Registry of Transplant Recipients registry data were integrated with national pharmaceutical claims (2007-2016) to identify HCV treatments before January 2014 (pre-DAA) and after (post-DAA), stratified by donor (D) and recipient (R) serostatus and payer. Pre-DAA, 18% of HCV+ LT recipients were treated within 3 years and without differences by donor serostatus or payer. Post-DAA, only 6% of D-/R+ recipients, 19.8% of D+/R+ recipients with public insurance, and 11.3% with private insurance were treated within 3 years (P < .0001). LT recipients treated for HCV pre-DAA experienced higher rates of graft loss (adjusted hazard ratio [aHR] 1.34 1.852.10 , P < .0001) and death (aHR 1.47 1.681.91 , P < .0001). Post-DAA, HCV treatment was not associated with death (aHR 0.34 0.671.32 , P = .25) or graft failure (aHR 0.32 0.641.26 , P = .20) in D+R+ LT recipients. Treatment increased in D+R+ KT recipients (5.5% pre-DAA vs 12.9% post-DAA), but did not differ by payer status. DAAs reduced the risk of death after D+/R+ KT by 57% (0.19 0.430.95 , P = .04) and graft loss by 46% (0.27 0.541.07 , P = .08). HCV treatment with DAAs appears to improve HCV+ LT and KT outcomes; however, access to these medications appears limited in both LT and KT recipients.
Keywords: clinical research/practice; economics; health services and outcomes research; infection and infectious agents - viral: hepatitis C; kidney (allograft) function/dysfunction; kidney transplantation/nephrology; liver allograft function/dysfunction; liver transplantation/hepatology; patient survival.
© 2018 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
Comment in
-
If hepatitis C therapy is so great, why isn't everyone doing it?Am J Transplant. 2018 Oct;18(10):2382-2383. doi: 10.1111/ajt.14960. Epub 2018 Jun 22. Am J Transplant. 2018. PMID: 29862650 No abstract available.
References
-
- Charlton M, Everson GT, Flamm SL, et al. Ledipasvir and Sofosbuvir Plus Ribavirin for Treatment of HCV Infection in Patients With Advanced Liver Disease. Gastroenterology. 2015;149(3):649–659. - PubMed
-
- Alqahtani SA, Afdhal N, Zeuzem S, et al. Safety and tolerability of ledipasvir/sofosbuvir with and without ribavirin in patients with chronic hepatitis C virus genotype 1 infection: Analysis of phase III ION trials. Hepatology. 2015;62(1):25–30. - PubMed
-
- Reddy KR, Bourliere M, Sulkowski M, et al. Ledipasvir and sofosbuvir in patients with genotype 1 hepatitis C virus infection and compensated cirrhosis: An integrated safety and efficacy analysis. Hepatology. 2015;62(1):79–86. - PubMed
-
- Curry MP, O’Leary JG, Bzowej N, et al. Sofosbuvir and Velpatasvir for HCV in Patients with Decompensated Cirrhosis. The New England journal of medicine. 2015;373(27):2618–2628. - PubMed
-
- Cheung MCM, Walker AJ, Hudson BE, et al. Outcomes after successful direct-acting antiviral therapy for patients with chronic hepatitis C and decompensated cirrhosis. Journal of hepatology. 2016;65(4):741–747. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
