

Comparing the Diagnostic Accuracy of Ultrasound and CT in Evaluating Acute Cholecystitis
- PMID: 29702020
- PMCID: PMC6082629
- DOI: 10.2214/AJR.17.18884
Comparing the Diagnostic Accuracy of Ultrasound and CT in Evaluating Acute Cholecystitis
Abstract
Objective: In 2013, a multidisciplinary group at our Veterans Administration hospital collaborated to improve the diagnosis and treatment of patients with acute cholecystitis (AC) at our facility. Our role in this project was to evaluate the diagnostic accuracies of ultrasound (US) and CT.
Materials and methods: AC was diagnosed in 60 patients (62 patient encounters) between July 1, 2013, and July 1, 2015. Of these patients, 56 underwent US, 48 underwent CT, and 42 underwent both. For the same time period, 60 patients without AC underwent US and 60 patients without AC underwent CT, and these imaging studies served as comparison studies. The groups were combined for a total of 182 unique patient encounters. A single radiologist reviewed the studies and tabulated the data.
Results: The sensitivity of CT for detecting AC was significantly greater than that of US: 85% versus 68% (p = 0.043), respectively; however, the negative predictive values of CT and US did not differ significantly: 90% versus 77% (p = 0.24-0.26). Because there were no false-positives, the specificity and positive predictive values for both modalities were 100%. Among the 42 patients who underwent CT and US, both modalities were positive for AC in 25 patients, CT was positive and US was negative in 10 patients, and US was positive and CT was negative in two patients; in five patients, both US and CT were negative.
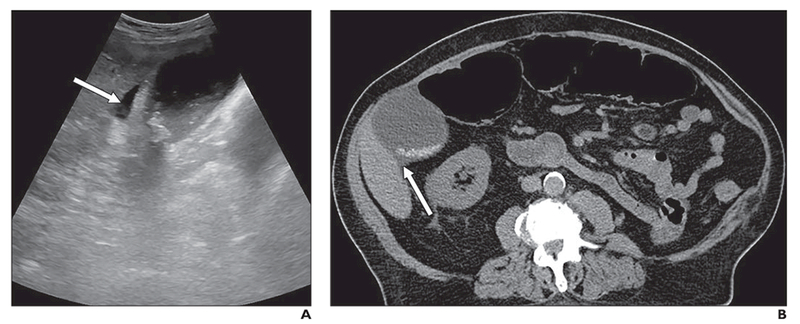
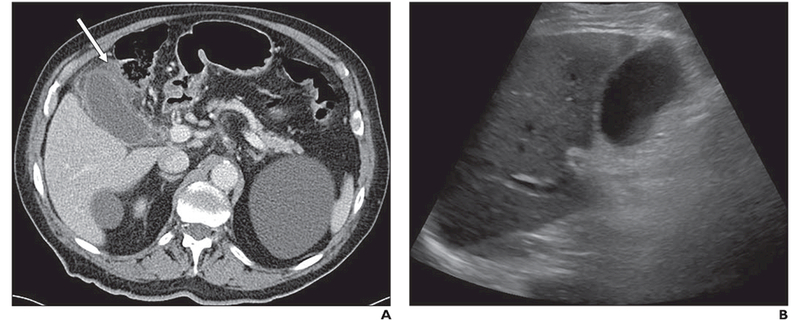
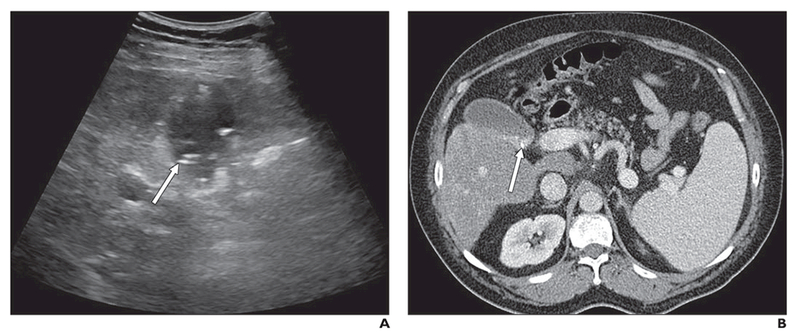
Conclusion: CT was significantly more sensitive for diagnosing AC than US. CT and US are complementary, and the other modality should be considered if there is high clinical suspicion for AC and the results of the first examination are negative.
Keywords: CT; Veterans Administration medical center; acute cholecystitis; quality improvement; ultrasound.
Figures
Comment in
-
Reply to "Diagnosis of Acute Cholecystitis: Clinical, Radiologic, or Both?".AJR Am J Roentgenol. 2018 Oct;211(4):W204. doi: 10.2214/AJR.18.20176. AJR Am J Roentgenol. 2018. PMID: 30240316 No abstract available.
-
Diagnosis of Acute Cholecystitis: Clinical, Radiologic, or Both?AJR Am J Roentgenol. 2018 Oct;211(4):W203. doi: 10.2214/AJR.18.20105. AJR Am J Roentgenol. 2018. PMID: 30240322 No abstract available.
-
Ultrasound Versus CT for the Diagnosis of Acute Cholecystitis.AJR Am J Roentgenol. 2019 Feb;212(2):W43. doi: 10.2214/AJR.18.20440. AJR Am J Roentgenol. 2019. PMID: 30667312 No abstract available.
-
Reply to "Ultrasound Versus CT for the Diagnosis of Acute Cholecystitis".AJR Am J Roentgenol. 2019 Feb;212(2):W44. doi: 10.2214/AJR.18.20540. AJR Am J Roentgenol. 2019. PMID: 30667315 No abstract available.
References
-
- Shakespear JS, Shaaban AM, Rezvani M. CT findings of acute cholecystitis and its complications. AJR 2010; 194:1523–1529 - PubMed
-
- Hanbidge AE, Buckler PM, O’Malley ME, Wilson SR. From the RSNA refresher courses: imaging evaluation for acute pain in the right upper quadrant. Radio Graphics 2004; 24:1117–1135 - PubMed
-
- Charalel RA, Jeffrey RB, Shin LK. Complicated cholecystitis: the complementary roles of sonography and computed tomography. Ultrasound Q 2011; 27:161–170 - PubMed
-
- Marincek B Nontraumatic abdominal emergencies: acute abdominal pain—diagnostic strategies. Eur Radiol 2002; 12:2136–2150 - PubMed
-
- Menu Y, Vuillerme MP. Non-traumatic abdominal emergencies: imaging and intervention in acute biliary conditions. Eur Radiol 2002; 12:2397–2406 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
