

Advances in Management of Esophageal Motility Disorders
- PMID: 29702296
- PMCID: PMC6317712
- DOI: 10.1016/j.cgh.2018.04.026
Advances in Management of Esophageal Motility Disorders
Abstract
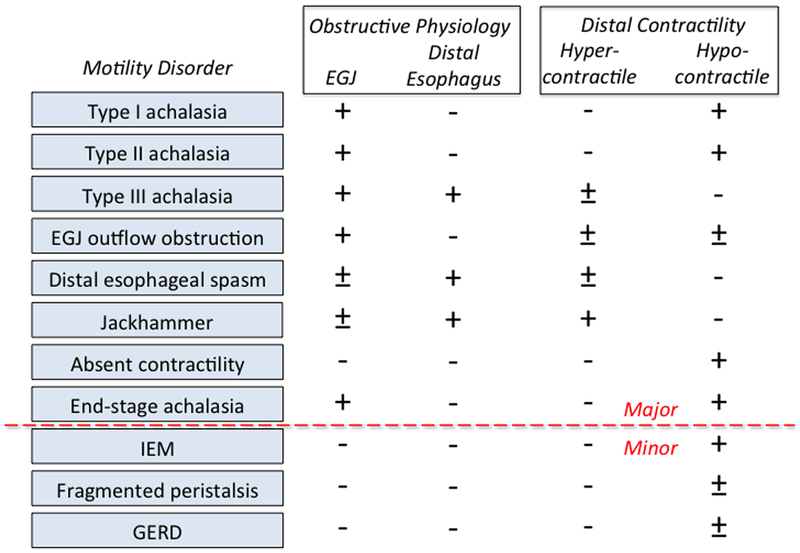
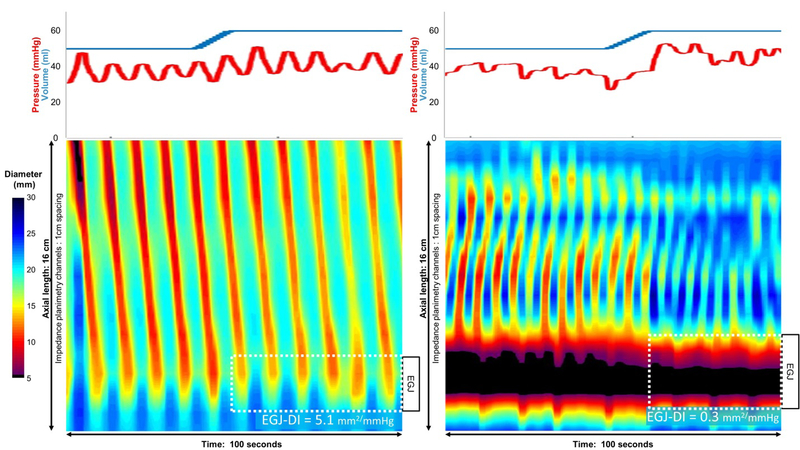
The widespread adoption of high-resolution manometry (HRM) has led to a restructuring in the classification of esophageal motility disorder classification summarized in the Chicago Classification, currently in version 3.0. It has become apparent that the cardinal feature of achalasia, impaired lower esophageal sphincter relaxation, can occur in several disease phenotypes: without peristalsis, with premature (spastic) distal esophageal contractions, with panesophageal pressurization, or even with preserved peristalsis. Furthermore, despite these advances in diagnostics, no single manometric pattern is perfectly sensitive or specific for idiopathic achalasia and complimentary assessments with provocative maneuvers during HRM or interrogating the esophagogastric junction with the functional luminal imaging probe during endoscopy can be useful in clarifying equivocal or inexplicable HRM findings. Using these tools, we have come to conceptualize esophageal motility disorders as characterized by obstructive physiology at the esophagogastric junction, smooth muscle esophagus, or both. Recognizing obstructive physiology as a primary target of therapy has become particularly relevant with the development of a minimally invasive technique for performing a calibrated myotomy of the esophageal circular muscle, the POEM procedure. Now and going forward, optimal management is to render treatment in a phenotype-specific manner: e.g. POEM calibrated to patient-specific physiology for spastic achalasia and spastic disorders of the smooth muscle esophagus, more conservative strategies (pneumatic dilation) for the disorders limited to the sphincter.
Keywords: Dysphagia; Esophageal Motility Disorders; Esophagus; High-Resolution Manometry.
Copyright © 2018 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Potential conflicts of interest
Peter J Kahrilas: No potential conflicts
Dustin A Carlson: No potential conflicts
John E Pandolfino: Medtronic, Sandhill, Torax; consulting and educational; Crospon; Stock Options
Figures
References
-
- Clouse RE, Staiano A. Topography of the esophageal peristaltic pressure wave. Am J Physiol 1991;261:G677–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
