

Primary functioning hepatic paraganglioma mimicking hepatocellular carcinoma: A case report and literature review
- PMID: 29702975
- PMCID: PMC5944498
- DOI: 10.1097/MD.0000000000010293
Primary functioning hepatic paraganglioma mimicking hepatocellular carcinoma: A case report and literature review
Abstract
Introduction: Hepatic paraganglioma (HPGL) originates from the sympathetic nervous tissue in the liver, and is an extremely rare type of the sympathetic paragangliomas. Till now, only 11 HPGL cases have been reported.
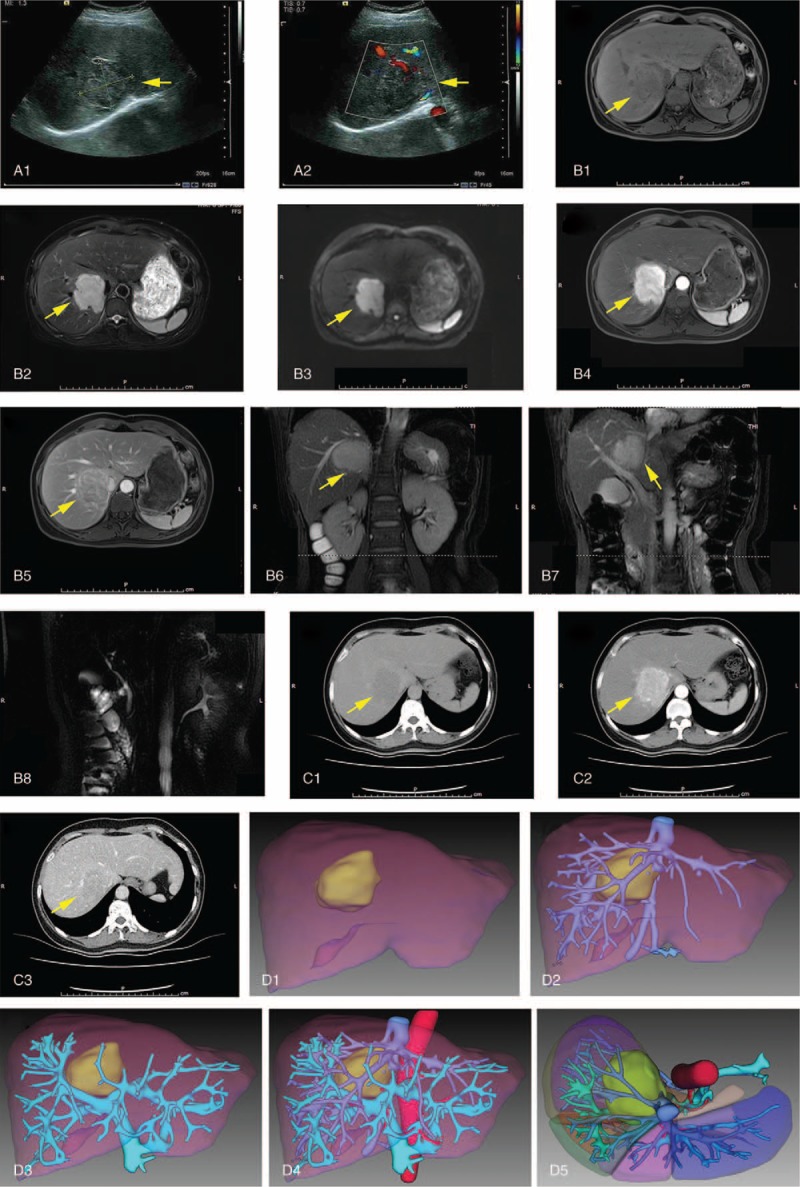
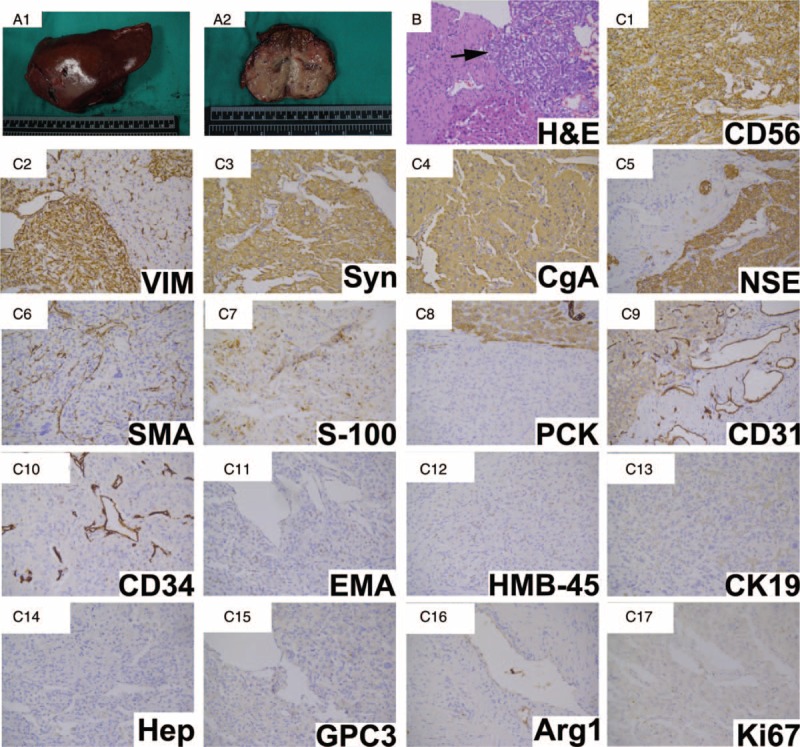
Case presentation: A 49-year-old woman presented to our hospital with a lesion in the right lobe of the liver, which grew from 2 to 6 cm in 2 years. In addition, she had a 6-year history of diabetes. The patient was initially diagnosed as hepatocellular carcinoma and hepatectomy was performed. Surgical resection of the liver lesion was successful, but the blood pressure rose and fell sharply when the lesion was being removed. The pathological examination of the liver lesion showed that it was HPGL. After the operation, the patient recovered uneventfully. Follow-up examination showed the blood glucose level went back to the normal range in 20 days after the operation, and MRI and I-MIBG scan showed that there was no evidence of recurrence and metastasis in >2 years.
Conclusion: By means of reporting this case and reviewing 11 reported cases, we conclude that the incidence of HPGLs is extremely low and the clinical and radiological characteristics of HPGLs are nonspecific; thus, it is hard to diagnose HPGLs correctly. Surgical resection is curative therapy for HPGLs, whereas the removing of HPGLs may cause the releasing of catecholamine, and then lead to hypertension crisis and arrhythmia. Thus, antihypertensive therapy is necessary during the operation. Follow-ups after the operation are important for HPGL patients, for pathological examinations are not sufficient to differ malignant HPGLs from benign ones, and follow-ups are helpful for HPGL patients to find the recurrent foci or metastases timely.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Primary hepatic paraganglioma mimicking hepatocellular carcinoma: a case report.Transl Cancer Res. 2022 Sep;11(9):3434-3439. doi: 10.21037/tcr-22-314. Transl Cancer Res. 2022. PMID: 36237251 Free PMC article.
-
Case Report: Unveiling an anomalous diaphragmatic paraganglioma mimicking a hepatic tumor.F1000Res. 2024 Oct 25;13:1023. doi: 10.12688/f1000research.155205.2. eCollection 2024. F1000Res. 2024. PMID: 39649836 Free PMC article.
-
Hepatic metastatic paraganglioma 12 years after retroperitoneal paraganglioma resection: a case report.BMC Gastroenterol. 2019 Aug 8;19(1):142. doi: 10.1186/s12876-019-1061-6. BMC Gastroenterol. 2019. PMID: 31395026 Free PMC article.
-
Malignant extra-adrenal pancreatic paraganglioma: case report and literature review.BMC Cancer. 2013 Oct 20;13:486. doi: 10.1186/1471-2407-13-486. BMC Cancer. 2013. PMID: 24138700 Free PMC article. Review.
-
Haemorrhagic retroperitoneal paraganglioma initially manifesting as acute abdomen: a rare case report and literature review.BMC Surg. 2020 Nov 30;20(1):304. doi: 10.1186/s12893-020-00953-y. BMC Surg. 2020. PMID: 33256692 Free PMC article. Review.
Cited by
-
Hepatic paraganglioma hiding as a slowly growing lesion for 24 years: a diagnostic conundrum.BMJ Case Rep. 2019 Mar 22;12(3):e228947. doi: 10.1136/bcr-2018-228947. BMJ Case Rep. 2019. PMID: 30904897 Free PMC article. No abstract available.
-
The Complex Histopathological and Immunohistochemical Spectrum of Neuroendocrine Tumors-An Overview of the Latest Classifications.Int J Mol Sci. 2023 Jan 11;24(2):1418. doi: 10.3390/ijms24021418. Int J Mol Sci. 2023. PMID: 36674939 Free PMC article. Review.
-
Paraganglioma masquerading as a primary liver lesion: A rare entity discovered during surgery.Clin Case Rep. 2022 Jan 25;10(1):e05310. doi: 10.1002/ccr3.5310. eCollection 2022 Jan. Clin Case Rep. 2022. PMID: 35106168 Free PMC article.
-
The Diagnosis and Clinical Significance of Paragangliomas in Unusual Locations.J Clin Med. 2018 Sep 13;7(9):280. doi: 10.3390/jcm7090280. J Clin Med. 2018. PMID: 30217041 Free PMC article. Review.
-
Tumour to tumour metastasis: case of a carotid body paraganglioma metastatic to a hepatocellular adenoma.BMJ Case Rep. 2022 Mar 2;15(3):e248527. doi: 10.1136/bcr-2021-248527. BMJ Case Rep. 2022. PMID: 35236704 Free PMC article.
References
-
- Favier J, Amar L, Gimenez-Roqueplo AP. Paraganglioma and phaeochromocytoma: from genetics to personalized medicine. Nat Rev Endocrinol 2015;11:101–11. - PubMed
-
- Burnichon N, Buffet A, Gimenez-Roqueplo AP. Pheochromocytoma and paraganglioma: molecular testing and personalized medicine. Curr Opin Oncol 2016;28:5–10. - PubMed
-
- Corssmit EP, Romijn JA. Clinical management of paragangliomas. Eur J Endocrinol 2014;171:R231–43. - PubMed
-
- Baudin E, Habra MA, Deschamps F, et al. Therapy of endocrine disease: treatment of malignant pheochromocytoma and paraganglioma. Eur J Endocrinol 2014;171:R111–122. - PubMed
-
- Rimmelin A, Hartheiser M, Gangi A, et al. Primary hepatic pheochromocytoma. Eur Radiol 1996;6:82–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
