

The application of x-ray, computed tomography, and magnetic resonance imaging on 22 pediatric Langerhans cell histiocytosis patients with long bone involvement: A retrospective analysis
- PMID: 29702989
- PMCID: PMC5944563
- DOI: 10.1097/MD.0000000000010411
The application of x-ray, computed tomography, and magnetic resonance imaging on 22 pediatric Langerhans cell histiocytosis patients with long bone involvement: A retrospective analysis
Abstract
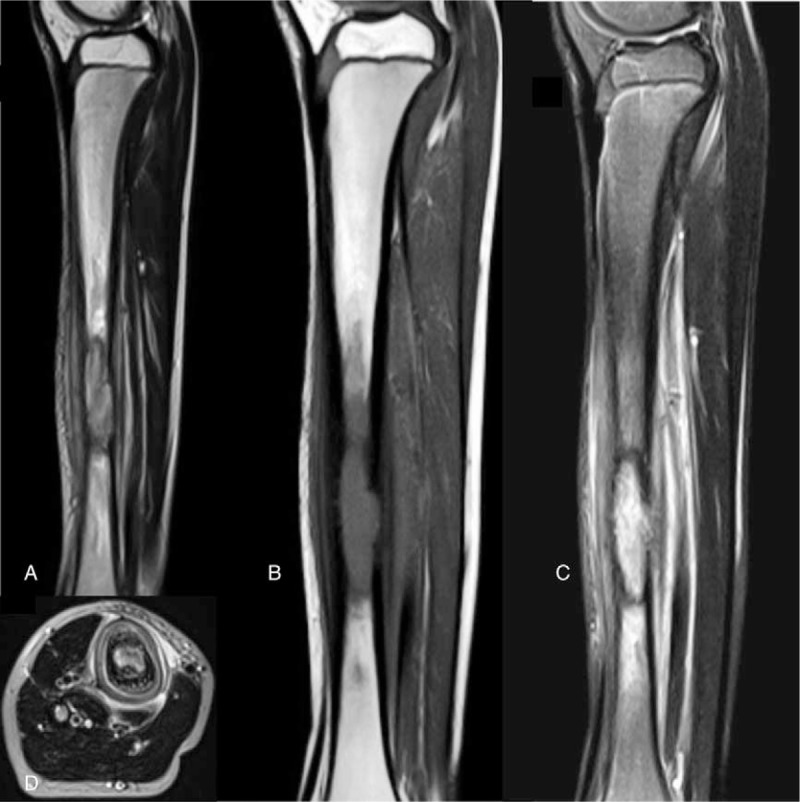
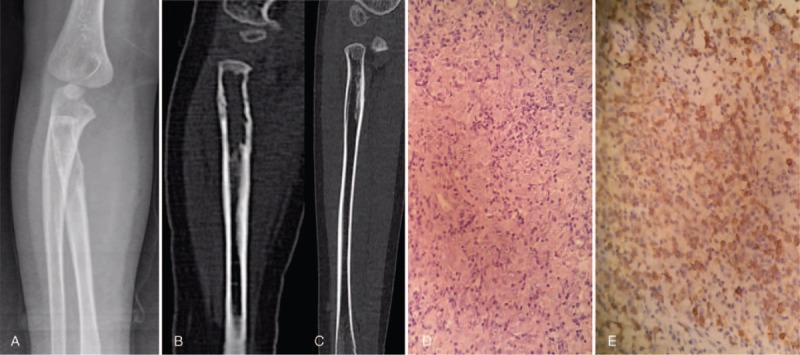
The studies focusing on x-ray, computed tomography (CT), and magnetic resonance imaging (MRI) in pediatric Langerhans cell histiocytosis (LCH) patients were still rare. Therefore, we aimed to evaluate the application of x-ray, CT, and MRI in pediatric LCH patients with long bone involvement.Total 22 pediatric LCH patients were included in this study. The diagnosis of LCH was confirmed by pathological examination. All patients were followed up for 3 years. X-ray, CT, or MRI was performed and the results were recorded for further analyses.Among 22 pediatric patients, x-ray (n = 20), CT (n = 18), or MRI (n = 12) were used to scan the lesion on long bones affected by LCH. Femurs (n = 13, 38.24%), tibia (n = 11, 32.35%), humerus (n = 5, 14.71%), and radius (n = 4, 11.76%) were the most frequently affected anatomic sites. Ovoid or round radiolucent lesions, aggressive periosteal reaction, and swelling of surrounding soft tissues were characteristic image of long bones on x-ray, CT, and MRI in pediatric LCH.Femurs, tibia, humerus, and radius were the most commonly affected long bones of pediatric LCH. The application of x-ray, CT, and MRI on long bones could help with the diagnosis of pediatric LCH.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
MRI and clinical features of Langerhans cell histiocytosis (LCH) in the pelvis and extremities: can LCH really look like anything?Skeletal Radiol. 2016 May;45(5):607-13. doi: 10.1007/s00256-016-2330-x. Epub 2016 Jan 22. Skeletal Radiol. 2016. PMID: 26802000
-
Clear cell chondrosarcoma: radiographic, computed tomographic, and magnetic resonance findings in 34 patients with pathologic correlation.Skeletal Radiol. 2003 Dec;32(12):687-94. doi: 10.1007/s00256-003-0668-3. Epub 2003 Oct 7. Skeletal Radiol. 2003. PMID: 14530882
-
Solid variant of aneurysmal bone cysts in long tubular bones: giant cell reparative granuloma.AJR Am J Roentgenol. 2003 Jun;180(6):1681-7. doi: 10.2214/ajr.180.6.1801681. AJR Am J Roentgenol. 2003. PMID: 12760943
-
Malignant transformation in monostotic fibrous dysplasia: clinical features, imaging features, outcomes in 10 patients, and review.Medicine (Baltimore). 2015 Jan;94(3):e369. doi: 10.1097/MD.0000000000000369. Medicine (Baltimore). 2015. PMID: 25621678 Free PMC article. Review.
-
Langerhans cell histiocytosis in sphenoid sinus with vision impairment: Case report and literature review.Sci Prog. 2024 Jul-Sep;107(3):368504241257129. doi: 10.1177/00368504241257129. Sci Prog. 2024. PMID: 39196602 Free PMC article. Review.
Cited by
-
The baseline metabolism parameters of 18F‑FDG PET/CT as promising prognostic biomarkers in pediatric Langerhans cell histiocytosis.Quant Imaging Med Surg. 2023 Sep 1;13(9):5934-5944. doi: 10.21037/qims-23-290. Epub 2023 Aug 4. Quant Imaging Med Surg. 2023. PMID: 37711802 Free PMC article.
-
Infantile BCG osteomyelitis ultimately diagnosed as a result of trauma.Radiol Case Rep. 2025 Jan 13;20(3):1784-1789. doi: 10.1016/j.radcr.2024.12.034. eCollection 2025 Mar. Radiol Case Rep. 2025. PMID: 39898337 Free PMC article.
-
18F-FDG PET/MR Assessment of Pediatric Langerhans Cell Histiocytosis.Int J Gen Med. 2021 Oct 1;14:6251-6259. doi: 10.2147/IJGM.S327134. eCollection 2021. Int J Gen Med. 2021. PMID: 34629891 Free PMC article.
-
Clinical characteristics and outcomes of Langerhans cell histiocytosis at a single institution in Thailand: a 20-year retrospective study.Asian Biomed (Res Rev News). 2021 Aug 20;15(4):171-181. doi: 10.2478/abm-2021-0022. eCollection 2021 Aug. Asian Biomed (Res Rev News). 2021. PMID: 37551332 Free PMC article.
-
Role of 18F-FDG PET/CT in the diagnosis and management of patients with Langerhans cell histiocytosis.Quant Imaging Med Surg. 2022 Jun;12(6):3351-3363. doi: 10.21037/qims-21-823. Quant Imaging Med Surg. 2022. PMID: 35655814 Free PMC article.
References
-
- Zinn DJ, Chakraborty R, Allen CE. Langerhans cell histiocytosis: emerging insights and clinical implications. Oncology (Williston Park) 2016;30:122–32. 139. - PubMed
-
- Stull MA, Kransdorf MJ, Devaney KO. Langerhans cell histiocytosis of bone. Radiographics 1992;12:801–23. - PubMed
-
- Wang J, Wu X, Xi ZJ. Langerhans cell histiocytosis of bone in children: a clinicopathologic study of 108 cases. World J Pediatr 2010;6:255–9. - PubMed
-
- Vadivelu S, Mangano FT, Miller CR, et al. Multifocal Langerhans cell histiocytosis of the pediatric spine: a case report and literature review. Childs Nerv Syst 2007;23:127–31. - PubMed
-
- Badalian-Very G, Vergilio JA, Fleming M, et al. Pathogenesis of langerhans cell histiocytosis. Annu Rev Pathol 2013;8:1–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
