

Association between perioperative hypothermia and patient outcomes after thoracic surgery: A single center retrospective analysis
- PMID: 29703025
- PMCID: PMC5944492
- DOI: 10.1097/MD.0000000000010528
Association between perioperative hypothermia and patient outcomes after thoracic surgery: A single center retrospective analysis
Abstract
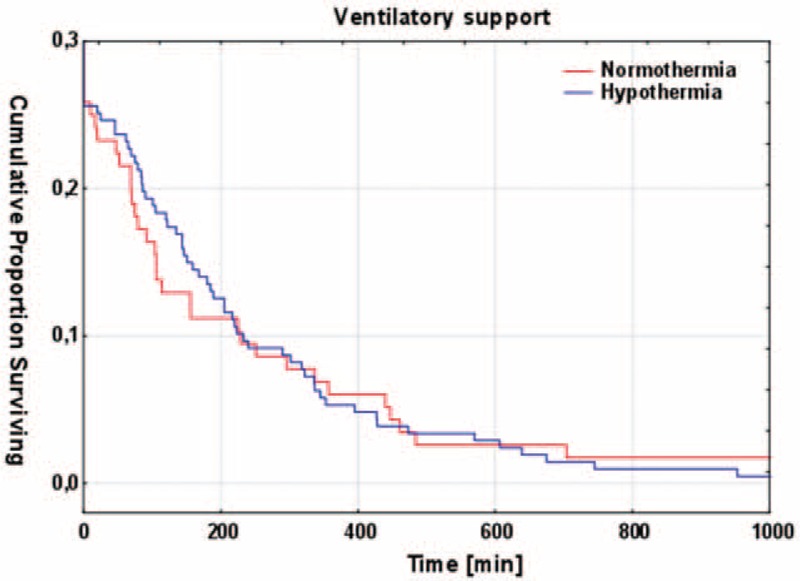
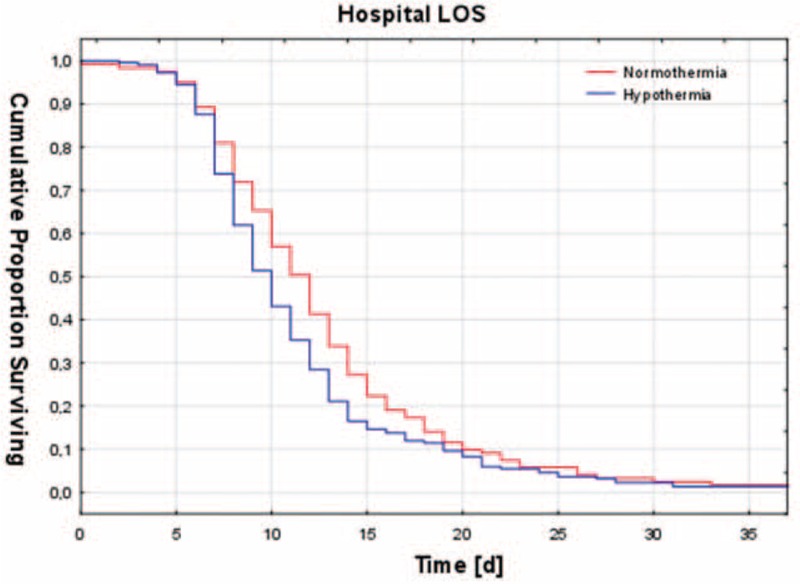
Hypothermia due to anaesthetic-induced impairment of thermoregulatory control and exposure to a cool environment is common in surgical patients. Peripheral vasodilation due to neuroaxial blockade may aggravate hypothermia. There is few data on perioperative hypothermia in patients undergoing thoracic surgery under combined general and regional anesthesia. We reviewed all thoracic surgical patients between 2006 and 2011 to determine the incidence and extent of hypothermia with or without an epidural anesthesia and evaluated its effect.Around 339 patients underwent lung resection procedures with intraoperative forced-air warming: 197 with general and epidural anesthesia (GA + EPI), 199 with general anesthesia alone (GA). Statistical analyses were performed to determine the association between hypothermia (T < 36°C) and transfusion requirements, length of stay (LOS) in the intensive care unit (ICU), hospital LOS, and in hospital mortality.The overall incidence of hypothermia was 64.3%. Multivariate regression analysis revealed three significant risk factors for the development of hypothermia: long induction time (P = .011), small body surface area (P = .003), and application of more fluid intraoperatively (P < .001). Factors determining the extent of hypothermia were: receiving an open thoracotomy (P = .009), placement and use of an epidural catheter (P = .002), and a lower body mass index (BMI) (P < .001). Additional epidural anesthesia reduced core temperature by 0.26°C (95% CI -0.414 to -0.095°C, P < .05). There was no difference in transfusion requirements, ICU LOS or mortality between both groups. Hospital LOS was longer in patients with hypothermia.More than half of all thoracic patients suffered from hypothermia. A long induction time, small body surface area, and large intraoperative fluid application were independent risk factors for the development of perioperative hypothermia. Additional epidural anesthesia to general anesthesia did not increase the incidence of hypothermia but decreased body core temperature to an-albeit not clinically significant-degree. Patients scheduled for thoracic surgery will probably benefit from an additional period of prewarming prior to induction to reduce the high incidence of perioperative hypothermia.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Aronoff DM, Neilson EG. Antipyretics: mechanisms of action and clinical use in fever suppression. Am J Med 2001;111:304–15. - PubMed
-
- National Institute for Health and Clinical Excellence Inadvertent perioperative hypothermia: The management of inadvertent perioperative hypothermia in adults having surgery [Internet]. [cited Apr. 2008; Last updated Dec. 2016]. Available at: https://www.nice.org.uk/guidance/cg65/evidence. Accessed October 8, 2016.
-
- Frank SM, Fleisher LA, Breslow MJ, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA 1997;277:1127–34. - PubMed
-
- Rajagopalan S, Mascha E, Na J, et al. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology 2008;108:71–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
