

Evaluation of a novel vital sign device to reduce maternal mortality and morbidity in low-resource settings: a mixed method feasibility study for the CRADLE-3 trial
- PMID: 29703254
- PMCID: PMC5924508
- DOI: 10.1186/s12884-018-1737-x
Evaluation of a novel vital sign device to reduce maternal mortality and morbidity in low-resource settings: a mixed method feasibility study for the CRADLE-3 trial
Abstract
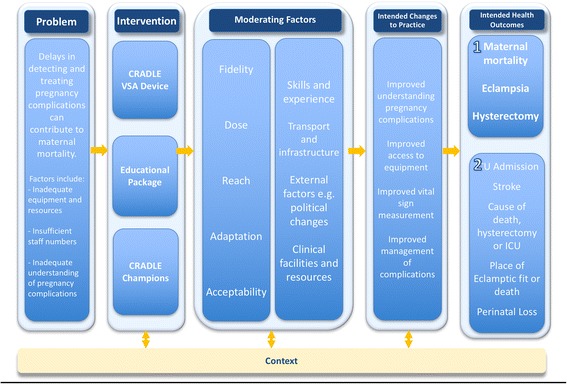
Background: The CRADLE-3 trial is a stepped-wedge randomised controlled trial aiming to reduce maternal mortality and morbidity by implementing a novel vital sign device (CRADLE Vital Sign Alert) and training package into routine maternity care in 10 low-income sites. The MRC Guidance on complex interventions proposes that interventions and implementation strategies be shaped by early phase piloting and development work. We present the findings of a three-month mixed-methodology feasibility study for this trial, describe how this was informed by the MRC guidance and the study design was refined.
Methods: The fidelity, dose, feasibility and acceptability of implementation and training materials were assessed in three representative non-trial sites (Zimbabwe, Ethiopia, India) using multiple-choice questionnaires, evaluation of clinical management (action log), healthcare provider (HCP) semi-structured interviews and focus groups 4-10 weeks after implementation. Simultaneously, the 10 sites included in the main trial (eight countries) collected primary outcome data to inform the power calculation and randomisation allocation and assess the feasibility of data collection.
Results: The package was implemented with high fidelity (85% of HCP trained, n = 204). The questionnaires indicated a good understanding of device use with 75% of participants scoring > 75% (n = 97; 90% of those distributed). Action logs were inconsistently completed but indicated that the majority of HCP responded appropriately to abnormal results. From 18 HCP interviews and two focus groups it was widely reported that the intervention improved capacity to make clinical decisions, escalate care and make appropriate referrals. Nine of the ten main trial sites achieved ethical approval for pilot data collection. Intensive care was an inconsistent marker of morbidity and stroke an infrequent outcome and therefore they were removed from the main trial composite outcome. Tools and methods of data collection were optimized and event rates used to inform randomisation.
Conclusions: This feasibility study demonstrates that the components of the intervention were acceptable, methods of implementing were successful and the main trial design would be feasible. Qualitative work identified key moderators that informed the main trial process evaluation. Changes to the training package, implementation strategy, study design and processes were identified to refine the implementation in the main trial.
Trial registration: ISRCTN41244132 ; Registered 24/11/2015.
Keywords: Complex intervention; Feasibility; Implementation; Low resource; Maternal mortality; Pilot.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval has been granted by the Biomedical Sciences, Dentistry, Medicine and Natural & Mathematical Sciences Research Ethics Subcommittee at King’s College London (LRS-14/15–1484). Local ethical approval from each cluster has been granted by:
Ethiopian Public Health Institute, Ethiopia: EPHI6.4/185
K.L.E Society’s Jawaharlal Nehru Medical College, Belgaum, India: MDC/IECHSR/2015–16/A-59
Medical Research Council of Zimbabwe; Zimbabwe: MRCZ/A/1999
Institutional level consent was sought prior to implementation of the CRADLE intervention. Informed written consent was sought from HCP participating in interviews, focus group discussions and the action logs of clinical practice.
Competing interests
The CRADLE VSA has been developed by Microlife with academic input from King’s College London and funding from Bill and Melinda Gates. The device is provided at manufacturing cost for this trial and is available to purchase at low cost to all LMIC. King’s College London receive no funds from the sale of devices to LMIC.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organisation. Trends in maternal mortality: 1990 to 2013. Estimates by WHO, UNICEF, UNFPA, the World Bank and the United Nations population division. 2015 http://apps.who.int/iris/bitstream/10665/194254/1/9789241565141_eng.pdf?.... [Accessed 20th November 2017].
-
- World Health Organisation. The world health report 2005: make every mother and child count, vol. 2005. Geneva: World Health Organization.
-
- Baker EC, van der Westhuizen A, Duhig KE, Shennan A. Can a low-resource-use blood pressure device impact on global maternal mortality? Hypertension in pregnancy : official journal of the International Society for the Study of Hypertension in Pregnancy. 2011;30(3):359–363. doi: 10.3109/10641950903026532. - DOI - PubMed
-
- Nathan HL, de Greeff A, Hezelgrave NL, Chappell LC, Shennan AH. An accurate semiautomated oscillometric blood pressure device for use in pregnancy (including pre-eclampsia) in a low-income and middle-income country population: the microlife 3AS1-2. Blood Press Monit. 2015;20(1):52–55. doi: 10.1097/MBP.0000000000000086. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
