

Disease burden, complication rates, and health-care costs of heparin-induced thrombocytopenia in the USA: a population-based study
- PMID: 29703336
- PMCID: PMC6437775
- DOI: 10.1016/S2352-3026(18)30046-2
Disease burden, complication rates, and health-care costs of heparin-induced thrombocytopenia in the USA: a population-based study
Abstract
Background: Heparin-induced thrombocytopenia can be a life-threatening and limb-threatening complication of heparin therapy. Incidence and complication rates of this condition have been extrapolated from studies with modest sample sizes, and despite the availability of therapeutic interventions the outcomes of heparin-induced thrombocytopenia are not well understood. We aimed to estimate disease burden, complication rates, and costs of heparin-induced thrombocytopenia in the USA.
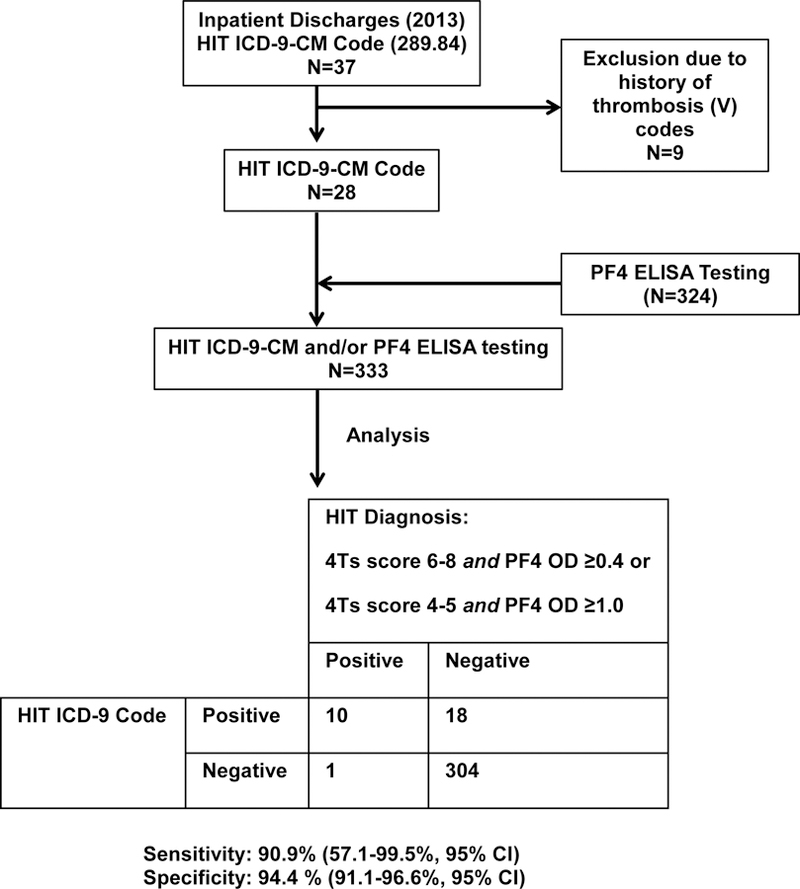
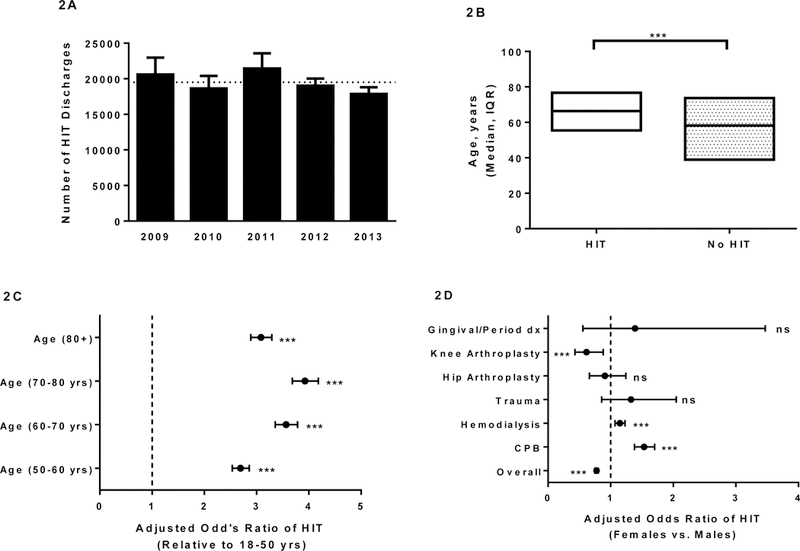
Methods: In this population-based study we analysed data from 2009 to 2013 from the Nationwide (National) Inpatient Sample (NIS), a large, all-payer inpatient health-care database in the USA. To validate the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code for heparin-induced thrombocytopenia (289.84), we defined the sensitivity and specificity of this code using patient data from 2013 from a local hospital (Froedtert Memorial Lutheran Hospital, Milwaukee, WI, USA). The primary outcomes assessed were the incidence of hospital discharges with codes for heparin-induced thrombocytopenia and of discharges for heparin-induced thrombocytopenia associated with cardiopulmonary bypass, haemodialysis, hip or knee arthroplasty, trauma or injury (or both), and gingival or periodontal disease (or both). We also assessed the incidence of thrombosis, bleeding, limb or digit amputation, mortality, length of hospital stay, and associated hospital charges.
Findings: Between 2009 and 2013, 97 566 discharges from the NIS assigned the ICD-9-CM code for heparin-induced thrombocytopenia, and 149 911 247 discharges coded for non-heparin-induced thrombocytopenia, were analysed. Overall, heparin-induced thrombocytopenia was identified in 97 566 (0·065%; SE 0·0012) of 150 008 813 discharges, corresponding to approximately one in 1500 hospital admissions. Patients undergoing cardiopulmonary bypass had the highest rates of heparin-induced thrombocytopenia (7702 [0·63%; SE 0·03] of 1 230 362), followed by those undergoing haemodialysis (23 012 [0·47%; 0·01] of 4 908 100), those with gingival or periodontal disease, or both (106 [0·12%; 0·03] of 88 621), and those with trauma or injury, or both (541 [0·09%; 0·01] of 602 944); patients with hip (845 [0·04%; 0·004] of 1 943 353) and knee (676 [0·02%; 0·002] of 3 022 602) arthroplasty had the lowest rates of heparin-induced thrombocytopenia. Thrombosis (29 079 [29·8%; SE 0·4] of 97 566) and bleeding (6044 [6·2%; 0·2] of 97 566) were common complications in heparin-induced thrombocytopenia, and 1446 (23·9%; 1·2) of 6044 patients with heparin-induced thrombocytopenia who had haemorrhage died. 742 (0·76%; SE 0·06) of 97 566 patients with heparin-induced thrombocytopenia discharges underwent amputations compared with 173 043 (0·12%; 0·001) of 149 911 247 with non-heparin-induced thrombocytopenia discharges (adjusted odds ratio 5·095 [95% CI 4·309-6·023]; p<0·0001). Overall, in-hospital mortality was 9842 (10·1%; SE 0·2) of 97 508 in discharge summaries coded for heparin-induced thrombocytopenia compared with 3 206 700 (2·1%; 0·01) of 149 811 891 in discharges for non-heparin-induced thrombocytopenia (adjusted odds ratio 4·075 [95% CI 3·846-4·317]; p<0·0001). The median length of stay among live discharges was 8·9 days (IQR 4·6-17·1) and total hospital charges were US$83 072 (IQR 37 240-188 419) for heparin-induced thrombocytopenia discharges compared with 2·6 days (1·4-4·8) and $21 360 (11 426-41 917) for non-heparin-induced thrombocytopenia discharges (p<0·0001 for both). 333 discharges from a local hospital were analysed to assess the diagnostic sensitivity and specificity of the heparin-induced thrombocytopenia ICD-9-CM code; sensitivity was 90·9% (95% CI 57·1-99·5) and specificity was 94·4% (91·1-96·6).
Interpretation: Complication rates for heparin-induced thrombocytopenia remain high and more effective preventive and treatment interventions are needed.
Funding: None.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of Interest
AP and RHA are listed as inventors on a patent related to HIT diagnostic testing (Patent Number. 9851367 [USPTO]. Pending in other jurisdictions). The other authors have no conflicts of interest to declare.
Figures




Comment in
-
Analysis of big data for heparin-induced thrombocytopenia: valuable information but also some doubts.Lancet Haematol. 2018 May;5(5):e188-e189. doi: 10.1016/S2352-3026(18)30050-4. Lancet Haematol. 2018. PMID: 29703334 No abstract available.
References
-
- Cuker A, Cines DB. How I treat heparin-induced thrombocytopenia. Blood 2012;119(10):2209–2218. - PubMed
-
- Morris TA, Castrejon S, Devendra G, Gamst AC. No difference in risk for thrombocytopenia during treatment of pulmonary embolism and deep venous thrombosis with either low-molecular-weight heparin or unfractionated heparin: a metaanalysis. Chest 2007;132(4):1131–1139. - PubMed
-
- Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced thrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin. N Engl J Med 1995;332(20):1330–1335. - PubMed
-
- Craik JD, Cobb AG. Heparin-induced thrombocytopenia following hip and knee arthroplasty. Br J Haematol 2013;161(2):255–261. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
