

Diagnosis and treatment of lipodystrophy: a step-by-step approach
- PMID: 29704234
- PMCID: PMC6304182
- DOI: 10.1007/s40618-018-0887-z
Diagnosis and treatment of lipodystrophy: a step-by-step approach
Abstract
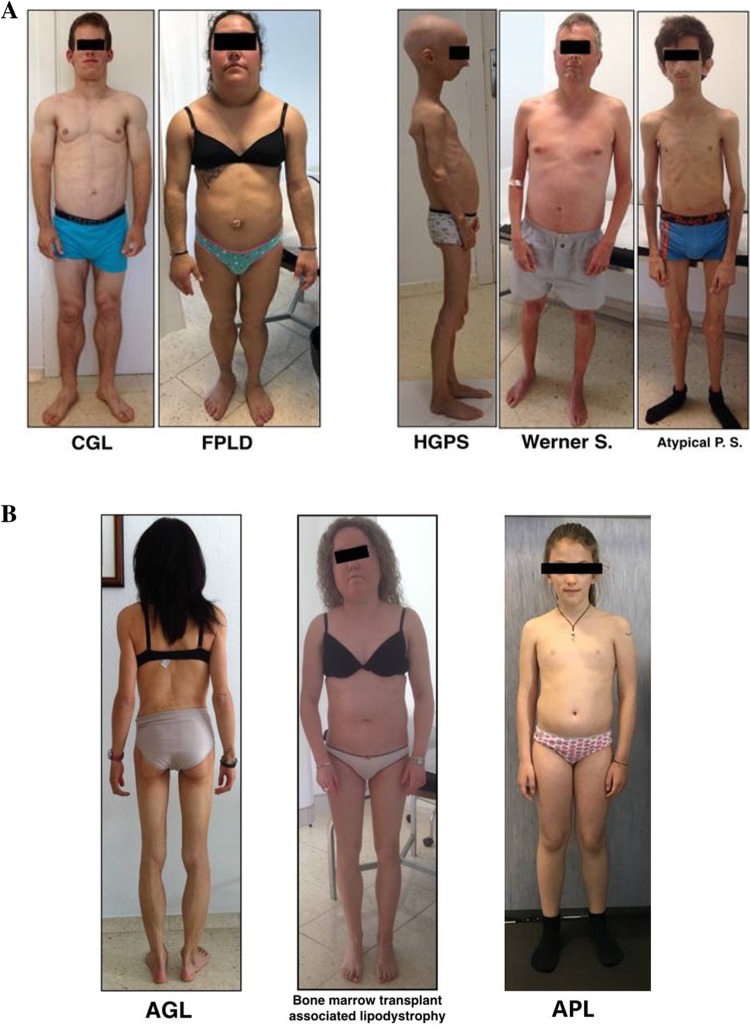
Aim: Lipodystrophy syndromes are rare heterogeneous disorders characterized by deficiency of adipose tissue, usually a decrease in leptin levels and, frequently, severe metabolic abnormalities including diabetes mellitus and dyslipidemia.
Purpose: To describe the clinical presentation of known types of lipodystrophy, and suggest specific steps to recognize, diagnose and treat lipodystrophy in the clinical setting.
Methods: Based on literature and in our own experience, we propose a stepwise approach for diagnosis of the different subtypes of rare lipodystrophy syndromes, describing its more frequent co-morbidities and establishing the therapeutical approach.
Results: Lipodystrophy is classified as genetic or acquired and by the distribution of fat loss, which can be generalized or partial. Genes associated with many congenital forms of lipodystrophy have been identified that may assist in diagnosis. Because of its rarity and heterogeneity, lipodystrophy may frequently be unrecognized or misdiagnosed, which is concerning because it is progressive and its complications are potentially life threatening. A basic diagnostic algorithm is proposed. Effective management of lipodystrophy includes lifestyle changes and aggressive, evidence-based treatment of comorbidities. Leptin replacement therapy (metreleptin) has been found to improve metabolic parameters in many patients with lipodystrophy. Metreleptin is approved in the United States as replacement therapy to treat the complications of leptin deficiency in patients with congenital or acquired generalized lipodystrophy and has been submitted for approval in Europe.
Conclusions: Here, we describe the clinical presentation of known types of lipodystrophy, present an algorithm for differential diagnosis of lipodystrophy, and suggest specific steps to recognize and diagnose lipodystrophy in the clinical setting.
Keywords: Diabetes; Dyslipidemia; Insulin resistance; Leptin replacement; Metreleptin.
Conflict of interest statement
Conflict of interest
David Araújo-Vilar and Ferruccio Santini have received honoraria as scientific advisors from Aegerion Pharmaceuticals.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
A written consent was obtained from the patients for the publication of their photographs.
Figures

References
-
- Brown RJ, Araujo-Vilar D, Cheung PT, Dunger D, Garg A, Jack M, Mungai L, Oral EA, Patni N, Rother KI, von Schnurbein J, Sorkina E, Stanley T, Vigouroux C, Wabitsch M, Williams R, Yorifuji T. The diagnosis and management of lipodystrophy syndromes: a multi-society practice guideline. J Clin Endocrinol Metab. 2016;101:4500–4511. doi: 10.1210/jc.2016-2466. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
