

Effective ventilation: The most critical intervention for successful delivery room resuscitation
- PMID: 29705089
- PMCID: PMC6288818
- DOI: 10.1016/j.siny.2018.04.001
Effective ventilation: The most critical intervention for successful delivery room resuscitation
Abstract
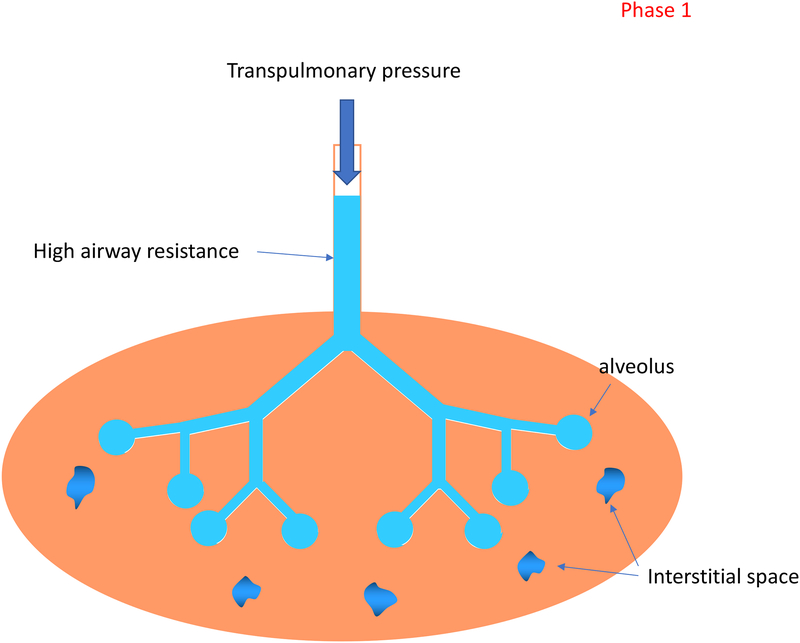
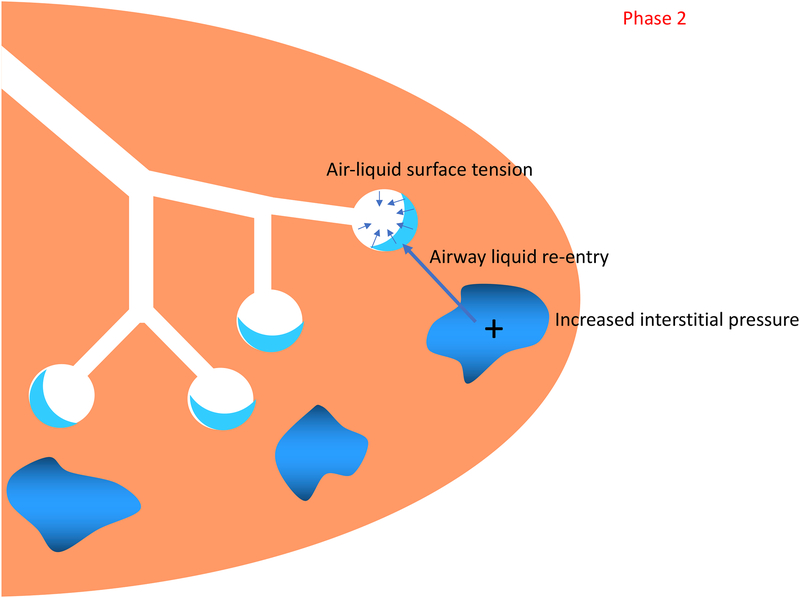
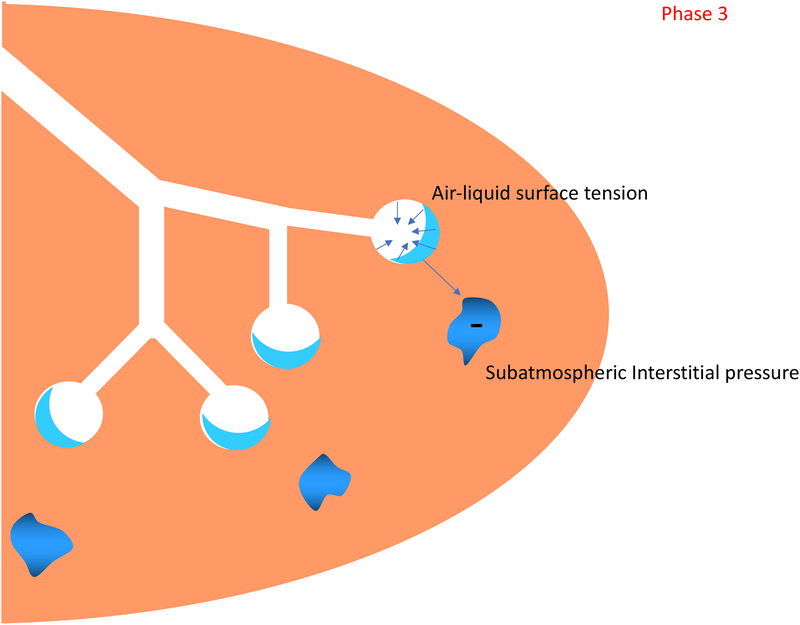
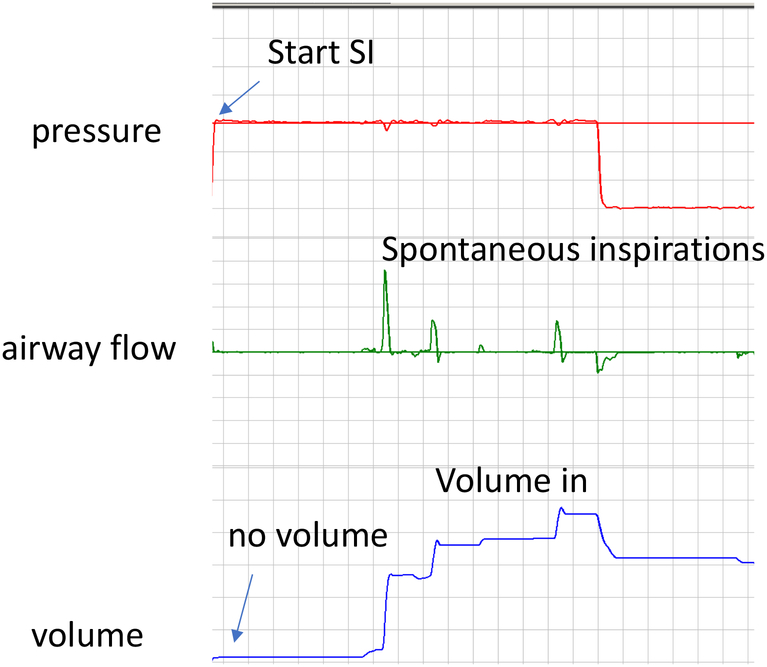
Lung aeration is the critical first step that triggers the transition from fetal to postnatal cardiopulmonary physiology after birth. When an infant is apneic or does not breathe sufficiently, intervention is needed to support this transition. Effective ventilation is therefore the cornerstone of neonatal resuscitation. In this article, we review the physiology of cardiopulmonary transition at birth, with particular attention to factors the caregiver should consider when providing ventilation. We then summarize the available clinical evidence for strategies to monitor and perform positive pressure ventilation in the delivery room setting.
Keywords: Lung aeration; Newborn; Resuscitation; Ventilation.
© 2018 Published by Elsevier Ltd.
Conflict of interest statement
Figures
Similar articles
-
Decrease in delivery room intubation rates after use of nasal intermittent positive pressure ventilation in the delivery room for resuscitation of very low birth weight infants.Resuscitation. 2017 Jul;116:33-38. doi: 10.1016/j.resuscitation.2017.05.004. Epub 2017 May 2. Resuscitation. 2017. PMID: 28476473
-
Practical procedures for the delivery room resuscitation of micropreemies.Semin Fetal Neonatal Med. 2022 Apr;27(2):101349. doi: 10.1016/j.siny.2022.101349. Epub 2022 Apr 30. Semin Fetal Neonatal Med. 2022. PMID: 35654729
-
Predictors of death including quality of positive pressure ventilation during newborn resuscitation and the relationship to outcome at seven days in a rural Tanzanian hospital.PLoS One. 2018 Aug 17;13(8):e0202641. doi: 10.1371/journal.pone.0202641. eCollection 2018. PLoS One. 2018. PMID: 30118519 Free PMC article.
-
Exhaled CO2 monitoring to guide non-invasive ventilation at birth: a systematic review.Arch Dis Child Fetal Neonatal Ed. 2023 Dec 15;109(1):74-80. doi: 10.1136/archdischild-2023-325698. Arch Dis Child Fetal Neonatal Ed. 2023. PMID: 37558397
-
Noninvasive Ventilation in the Delivery Room for the Preterm Infant.Neoreviews. 2019 Sep;20(9):e489-e499. doi: 10.1542/neo.20-9-e489. Neoreviews. 2019. PMID: 31477597 Review.
Cited by
-
Time to Effective Ventilation in Neonatal Manikins with a Supraglottic Airway vs. a Facemask: A Randomized Controlled Trial.Children (Basel). 2023 Mar 2;10(3):498. doi: 10.3390/children10030498. Children (Basel). 2023. PMID: 36980056 Free PMC article.
-
Neonatal Resuscitation Practices in Romania: A Survey of the Romanian Association of Neonatology (ANR) and the Union of European Neonatal and Perinatal Societies (UENPS).J Crit Care Med (Targu Mures). 2024 Jan 30;10(1):19-29. doi: 10.2478/jccm-2024-0010. eCollection 2024 Jan. J Crit Care Med (Targu Mures). 2024. PMID: 39108797 Free PMC article.
-
[Newborn resuscitation and support of transition of infants at birth].Notf Rett Med. 2021;24(4):603-649. doi: 10.1007/s10049-021-00894-w. Epub 2021 Jun 2. Notf Rett Med. 2021. PMID: 34093078 Free PMC article. Review. German.
-
Neonatal resuscitation practices in Italy: a survey of the Italian Society of Neonatology (SIN) and the Union of European Neonatal and Perinatal Societies (UENPS).Ital J Pediatr. 2022 Jun 2;48(1):81. doi: 10.1186/s13052-022-01260-3. Ital J Pediatr. 2022. PMID: 35655278 Free PMC article.
-
Effect of a positive pressure ventilation-refresher program on ventilation skill performance during simulated newborn resuscitation.Resusc Plus. 2021 Feb 16;5:100091. doi: 10.1016/j.resplu.2021.100091. eCollection 2021 Mar. Resusc Plus. 2021. PMID: 34223356 Free PMC article.
References
-
- Perlman JM, Wyllie J, Kattwinkel J, Wyckoff MH, Aziz K, Guinsburg R, et al. Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2015;132:S204–41. - PubMed
-
- Perlman JM, Risser R. Cardiopulmonary resuscitation in the delivery room. Associated clinical events. Arch Pediatr Adolesc Med 1995;149:20–5. - PubMed
-
- Hooper SB, Siew ML, Kitchen MJ, te Pas AB. Establishing functional residual capacity in the non-breathing infant. Semin Fetal Neonatal Med 2013;18:336–43. - PubMed
-
- Hooper SB, te Pas AB, Kitchen MJ. Respiratory transition in the newborn: a three-phase process. Arch Dis Child Fetal Neonatal Ed 2016:101:F266–71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
