

Systematic review of prediction models for delirium in the older adult inpatient
- PMID: 29705752
- PMCID: PMC5931306
- DOI: 10.1136/bmjopen-2017-019223
Systematic review of prediction models for delirium in the older adult inpatient
Abstract
Objective: To identify existing prognostic delirium prediction models and evaluate their validity and statistical methodology in the older adult (≥60 years) acute hospital population.
Design: Systematic review.
Data sources and methods: PubMed, CINAHL, PsychINFO, SocINFO, Cochrane, Web of Science and Embase were searched from 1 January 1990 to 31 December 2016. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses and CHARMS Statement guided protocol development.
Inclusion criteria: age >60 years, inpatient, developed/validated a prognostic delirium prediction model.
Exclusion criteria: alcohol-related delirium, sample size ≤50. The primary performance measures were calibration and discrimination statistics. Two authors independently conducted search and extracted data. The synthesis of data was done by the first author. Disagreement was resolved by the mentoring author.
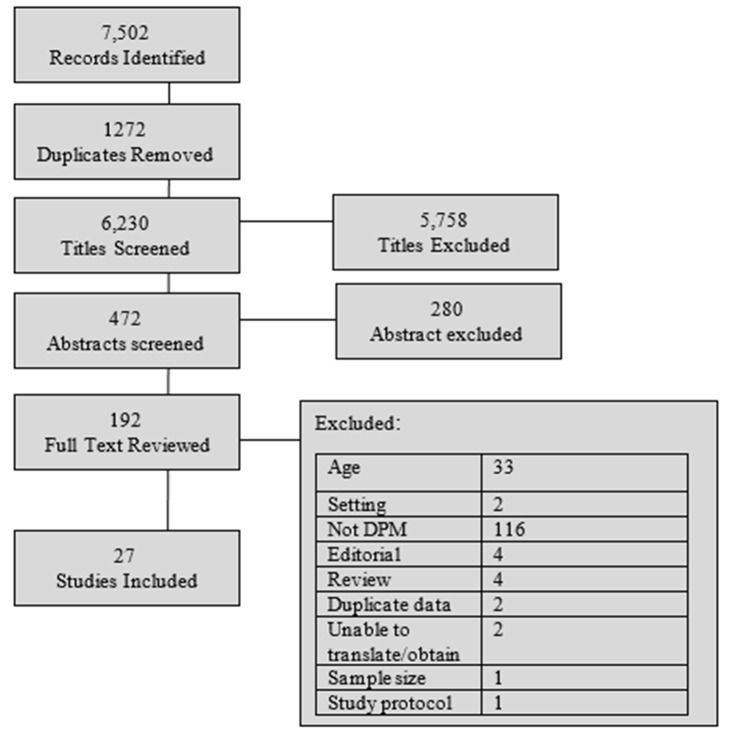
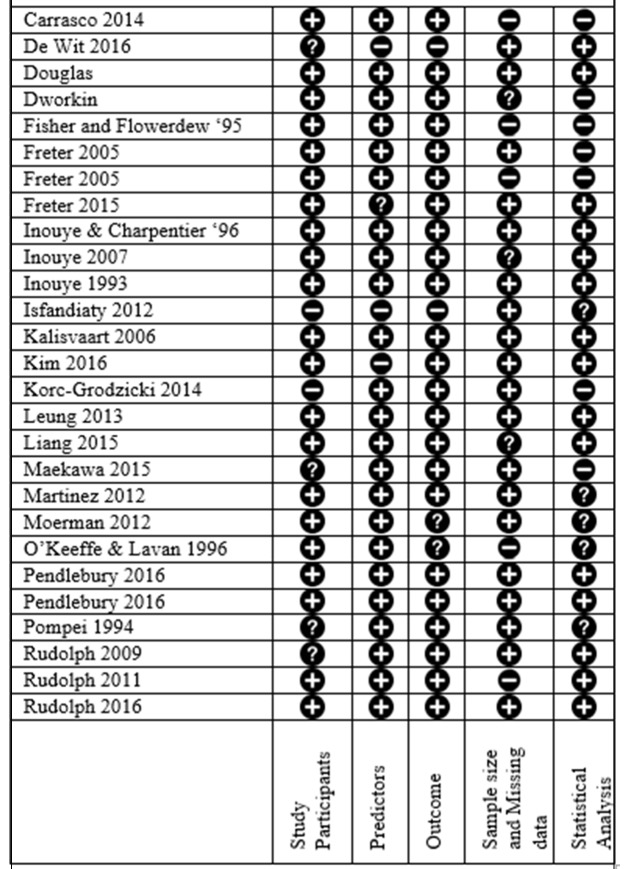
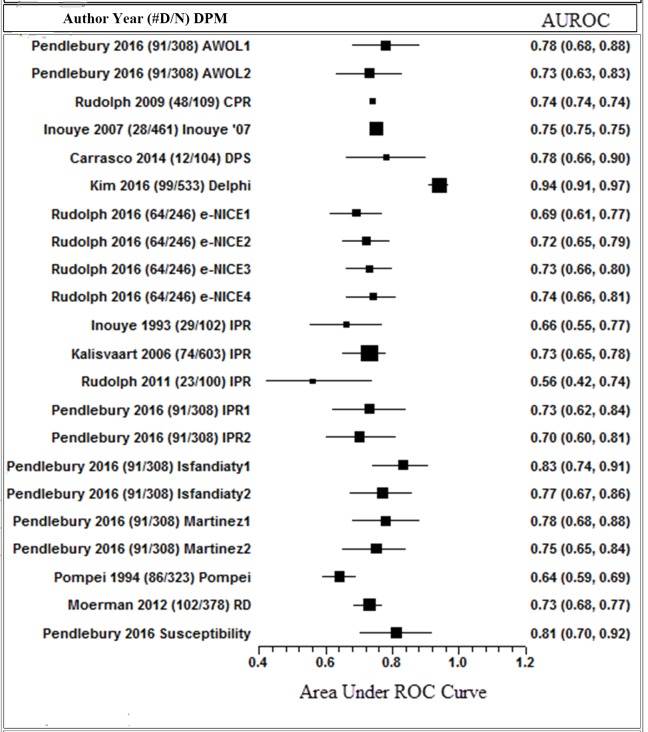
Results: The initial search resulted in 7,502 studies. Following full-text review of 192 studies, 33 were excluded based on age criteria (<60 years) and 27 met the defined criteria. Twenty-three delirium prediction models were identified, 14 were externally validated and 3 were internally validated. The following populations were represented: 11 medical, 3 medical/surgical and 13 surgical. The assessment of delirium was often non-systematic, resulting in varied incidence. Fourteen models were externally validated with an area under the receiver operating curve range from 0.52 to 0.94. Limitations in design, data collection methods and model metric reporting statistics were identified.
Conclusions: Delirium prediction models for older adults show variable and typically inadequate predictive capabilities. Our review highlights the need for development of robust models to predict delirium in older inpatients. We provide recommendations for the development of such models.
Keywords: delirium; geriatric medicine; statistic.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous