

Preoperative anemia versus blood transfusion: Which is the culprit for worse outcomes in cardiac surgery?
- PMID: 29706372
- PMCID: PMC6093299
- DOI: 10.1016/j.jtcvs.2018.03.109
Preoperative anemia versus blood transfusion: Which is the culprit for worse outcomes in cardiac surgery?
Abstract
Background: Reducing blood product utilization after cardiac surgery has become a focus of perioperative care as studies have suggested improved outcomes. The relative impact of preoperative anemia versus packed red blood cells (PRBC) transfusion on outcomes remains poorly understood, however. In this study, we investigated the relative association between preoperative hematocrit (Hct) level and PRBC transfusion on postoperative outcomes after coronary artery bypass grafting (CABG) surgery.
Methods: Patient records for primary, isolated CABG operations performed between January 2007 and December 2017 at 19 cardiac surgery centers were evaluated. Hierarchical logistic regression modeling was used to estimate the relationship between baseline preoperative Hct level as well as PRBC transfusion and the likelihoods of postoperative mortality and morbidity, adjusted for baseline patient risk. Variable and model performance characteristics were compared to determine the relative strength of association between Hct level and PRBC transfusion and primary outcomes.
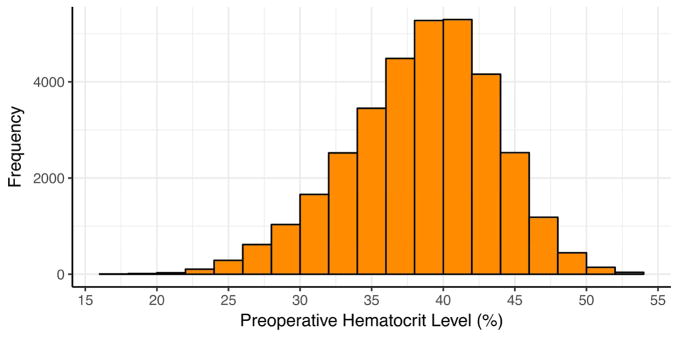
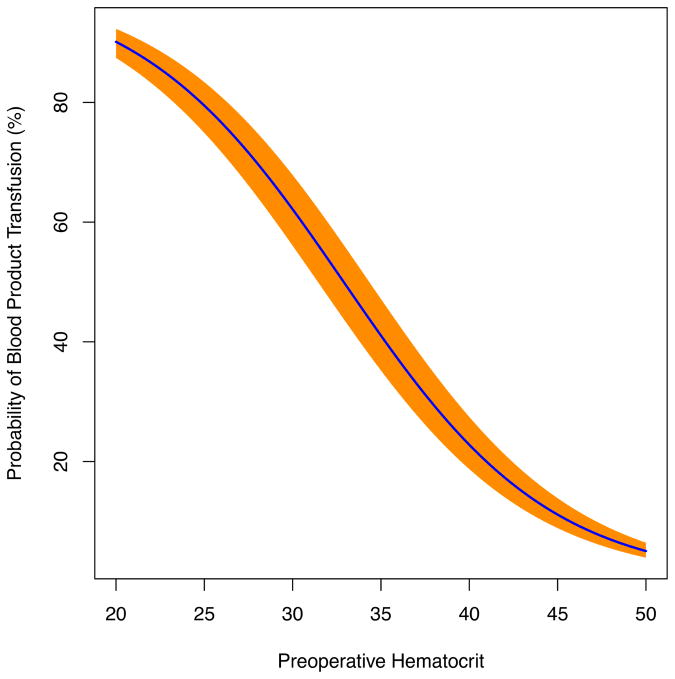
Results: A total of 33,411 patients (median patient age, 65 years; interquartile range [IQR], 57-72 years; 26% females) were evaluated. The median preoperative Hct value was 39% (IQR, 36%-42%), and the mean Society of Thoracic Surgeons (STS) predicted risk of mortality was 1.8 ± 3.1%. Complications included PRBC transfusion in 31% of patients, renal failure in 2.8%, stroke in 1.3%, and operative mortality in 2.0%. A strong association was observed between preoperative Hct value and the likelihood of PRBC transfusion (P < .001). After risk adjustment, PRBC transfusion, but not Hct value, demonstrated stronger associations with postoperative mortality (odds ratio [OR], 4.3; P < .0001), renal failure (OR 6.3; P < .0001), and stroke (OR, 2.4; P < .0001). A 1-point increase in preoperative Hct was associated with decreased probabilities of mortality (OR, 0.97; P = .0001) and renal failure (OR, 0.94; P < .0001). The models with PRBC had superior predictive power, with a larger area under the curve, compared with Hct for all outcomes (all P < .01). Preoperative anemia was associated with up to a 4-fold increase in the probability of PRBC transfusion, a 3-fold increase in renal failure, and almost double the mortality.
Conclusions: PRBC transfusion appears to be more closely associated with risk-adjusted morbidity and mortality compared with preoperative Hct level alone, supporting efforts to reduce unnecessary PRBC transfusions. Preoperative anemia independently increases the risk of postoperative morbidity and mortality. These data suggest that preoperative Hct should be included in the STS risk calculators. Finally, efforts to optimize preoperative hematocrit should be investigated as a potentially modifiable risk factor for mortality and morbidity.
Keywords: CABG; anemia; cardiac; hematocrit; transfusion.
Copyright © 2018 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author Conflicts of Interest: There are no potential author conflicts of interest
Figures


Comment in
-
Anemia, transfusion, and outcome: Both are bad…does it really matter which is worse?J Thorac Cardiovasc Surg. 2018 Jul;156(1):75-76. doi: 10.1016/j.jtcvs.2018.03.051. Epub 2018 Mar 26. J Thorac Cardiovasc Surg. 2018. PMID: 29655536 No abstract available.
-
Life imitates art far more than art imitates life-Oscar Wilde, "The Decay of Lying".J Thorac Cardiovasc Surg. 2018 Jul;156(1):64-65. doi: 10.1016/j.jtcvs.2018.03.082. Epub 2018 Mar 29. J Thorac Cardiovasc Surg. 2018. PMID: 29681400 No abstract available.
References
-
- Speiss BD. Transfusion and outcome in heart surgery. Ann Thorac Surg. 2002;74(4):986–987. - PubMed
-
- Stover EP, Siegel LC, Parks R, et al. Variability in transfusion practice for coronary artery bypass surgery persists despite national consensus guidelines: a 24-institution study. Institutions of the Multicenter Study of Perioperative Ischemia Research Group. Anesthesiology. 1998;88(2):327–333. - PubMed
-
- Banbury MK, Brizzio ME, Rajeswaran J, Lytle BW, Blackstone EH. Transfusion increases the risk of postoperative infection after cardiovascular surgery. J Am Coll Surg. 2006;202(1):131–138. - PubMed
-
- Engoren MC, Habib RH, Zacharias A, Schwann TA, Riordan CJ, Durham SJ. Effect of blood transfusion on long-term survival after cardiac operation. Ann Thorac Surg. 2002;74(4):1180–1186. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
