

Instrumental or Physical-Exercise Rehabilitation of Balance Improves Both Balance and Gait in Parkinson's Disease
- PMID: 29706993
- PMCID: PMC5863303
- DOI: 10.1155/2018/5614242
Instrumental or Physical-Exercise Rehabilitation of Balance Improves Both Balance and Gait in Parkinson's Disease
Abstract
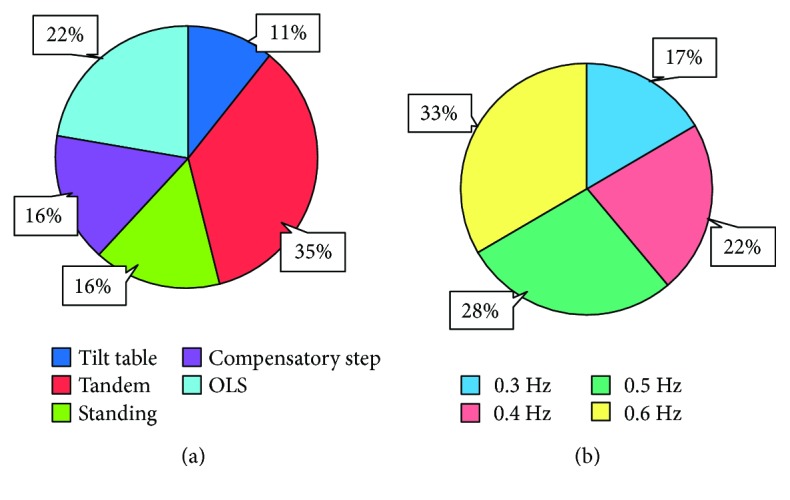
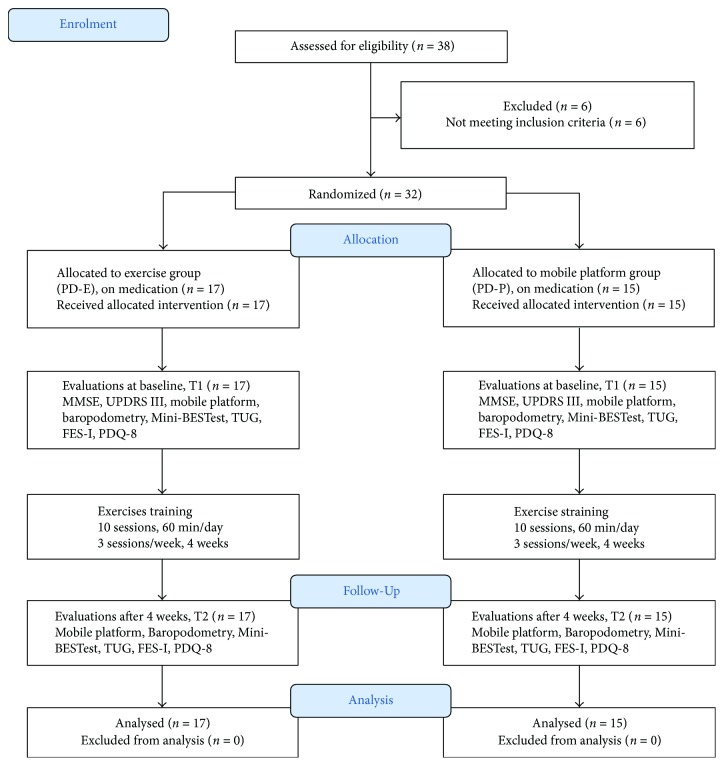
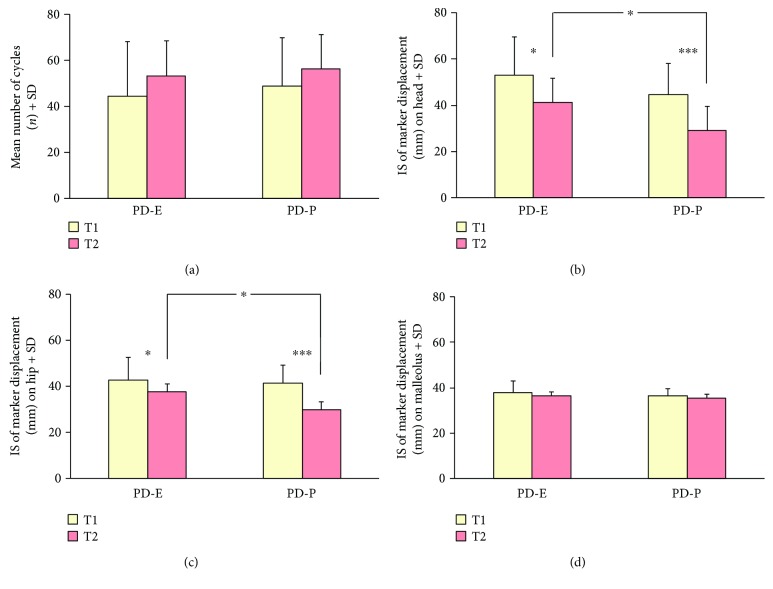
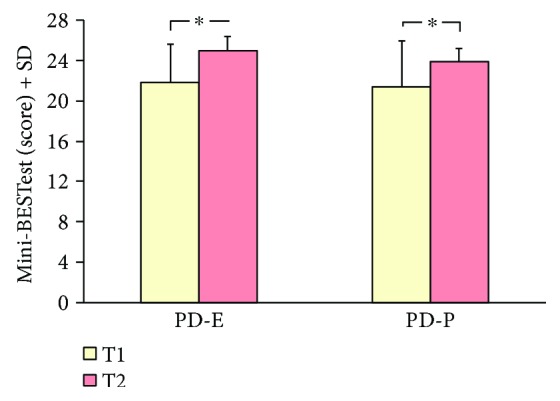
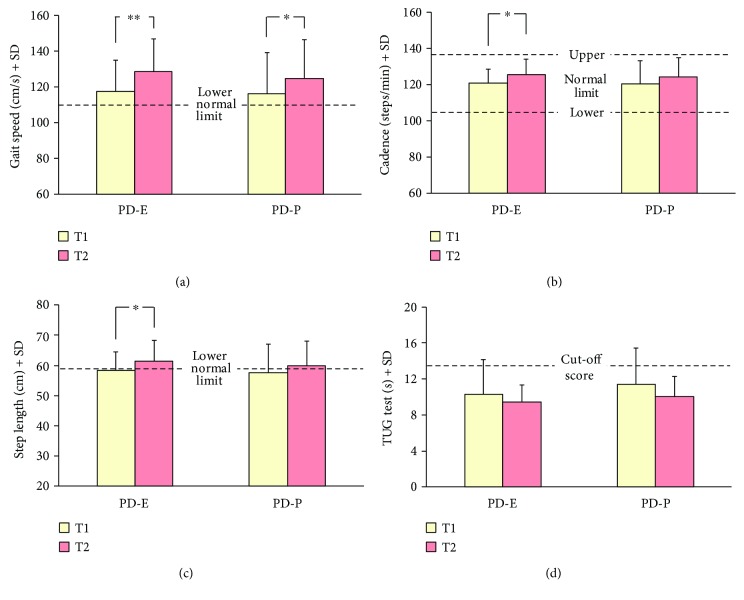
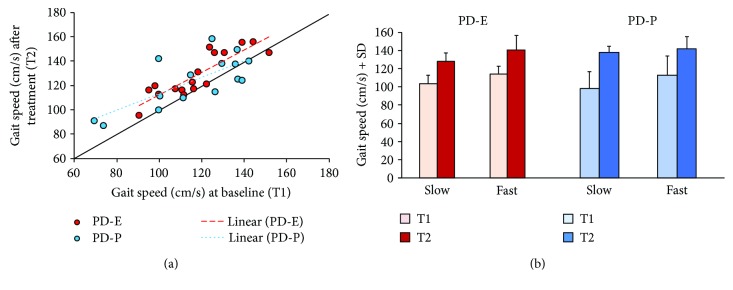
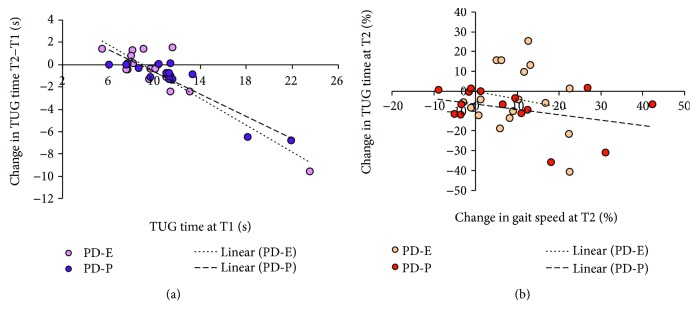
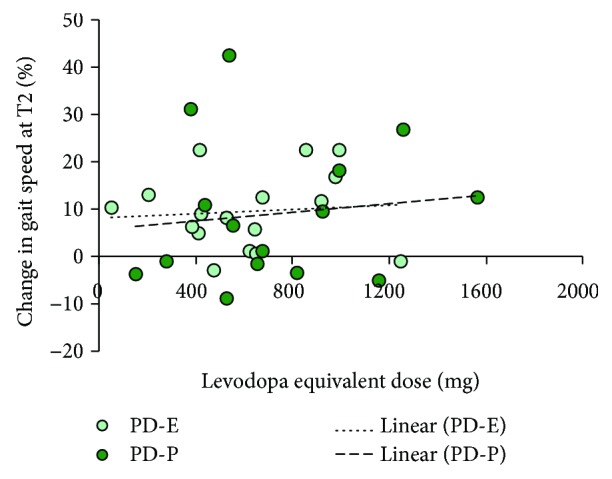
We hypothesised that rehabilitation specifically addressing balance in Parkinson's disease patients might improve not only balance but locomotion as well. Two balance-training protocols (standing on a moving platform and traditional balance exercises) were assessed by assigning patients to two groups (Platform, n = 15, and Exercises, n = 17). The platform moved periodically in the anteroposterior, laterolateral, and oblique direction, with and without vision in different trials. Balance exercises were based on the Otago Exercise Program. Both platform and exercise sessions were administered from easy to difficult. Outcome measures were (a) balancing behaviour, assessed by both Index of Stability (IS) on platform and Mini-BESTest, and (b) gait, assessed by both baropodometry and Timed Up and Go (TUG) test. Falls Efficacy Scale-International (FES-I) and Parkinson's Disease Questionnaire (PDQ-8) were administered. Both groups exhibited better balance control, as assessed both by IS and by Mini-BESTest. Gait speed at baropodometry also improved in both groups, while TUG was less sensitive to improvement. Scores of FES-I and PDQ-8 showed a marginal improvement. A four-week treatment featuring no gait training but focused on challenging balance tasks produces considerable gait enhancement in mildly to moderately affected patients. Walking problems in PD depend on postural instability and are successfully relieved by appropriate balance rehabilitation. This trial is registered with ClinicalTrials.gov NCT03314597.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
