

Age is major factor for predicting survival in patients with acute respiratory failure on extracorporeal membrane oxygenation: a Korean multicenter study
- PMID: 29707290
- PMCID: PMC5906318
- DOI: 10.21037/jtd.2018.03.71
Age is major factor for predicting survival in patients with acute respiratory failure on extracorporeal membrane oxygenation: a Korean multicenter study
Abstract
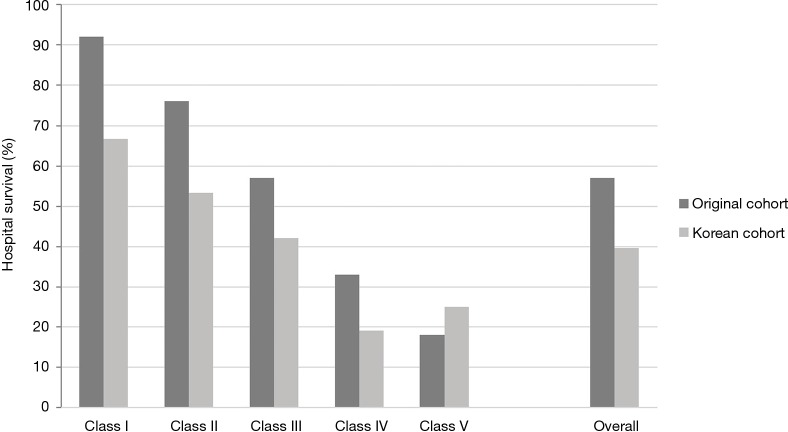
Background: The proportion of elderly patients in the intensive care unit population is increasing. Although the Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score is widely used for survival prediction of extracorporeal membrane oxygenation (ECMO) patients, it is questionable whether the RESP score is applicable to older patients. The aim of this study was to investigate the applicability of the RESP score in Korean cohort.
Methods: Data were retrospectively analyzed from 209 acute respiratory failure (ARF) patients treated with ECMO from 2014 to 2015 at 11 hospitals. A comparison of outcome prediction models was conducted and multivariate logistic regression analysis was performed to identify independent risk factors for hospital mortality.
Results: In all patients, the median age was 58 (IQR, 45-65) years. Overall survival at hospital discharge was 45.9%, and veno-venous ECMO was used in 82.3% of patients. Patients older than 65 years treated with ECMO support were 51 with 31.4% of hospital survival. The PRedicting dEath for SEvere ARDS on VV-ECMO (PRESERVE) and RESP scores significantly predicted mortality in patients, with areas under the curve (AUCs) of 0.63 [95% confidence interval (CI), 0.54-0.72] and 0.66 (95% CI, 0.58-0.73), respectively. In multivariate logistic regression analysis, age is independent risk factor for hospital mortality [odds ratio 1.044 (95% CI, 1.020-1.068), P<0.001] with AUC of 0.67 (95% CI, 0.59-0.74). The RESP score was modified using reclassified age and the modified RESP score obtained AUC of 0.71 (95% CI, 0.63-0.78).
Conclusions: The RESP score is significant model for predicting outcomes in a Korean ECMO population. Elderly patients had higher mortality, and age alone showed similar discrimination ability for prediction of mortality compared to the RESP score.
Keywords: Extracorporeal membrane oxygenation (ECMO); acute respiratory failure (ARF); age; survival.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures



References
LinkOut - more resources
Full Text Sources
Other Literature Sources