

Idiopathic subglottic stenosis: techniques and results
- PMID: 29707509
- PMCID: PMC5900086
- DOI: 10.21037/acs.2018.03.02
Idiopathic subglottic stenosis: techniques and results
Abstract
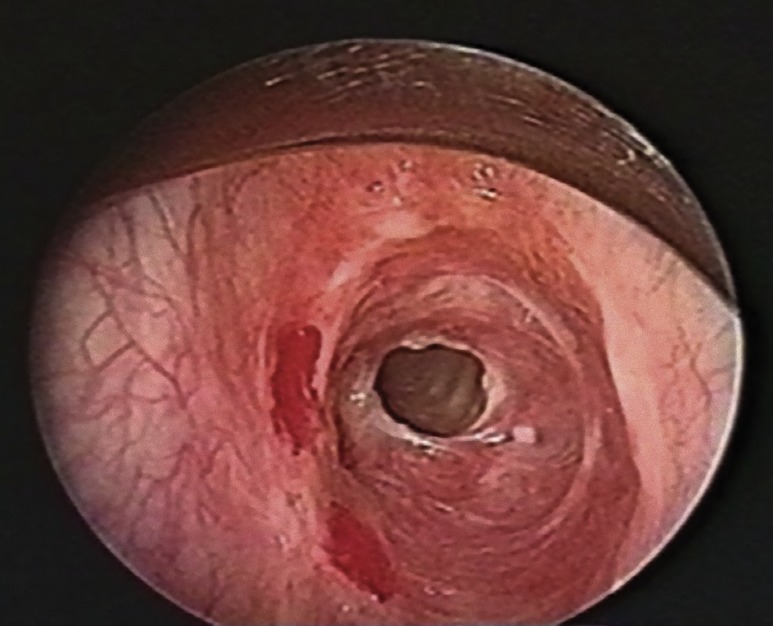
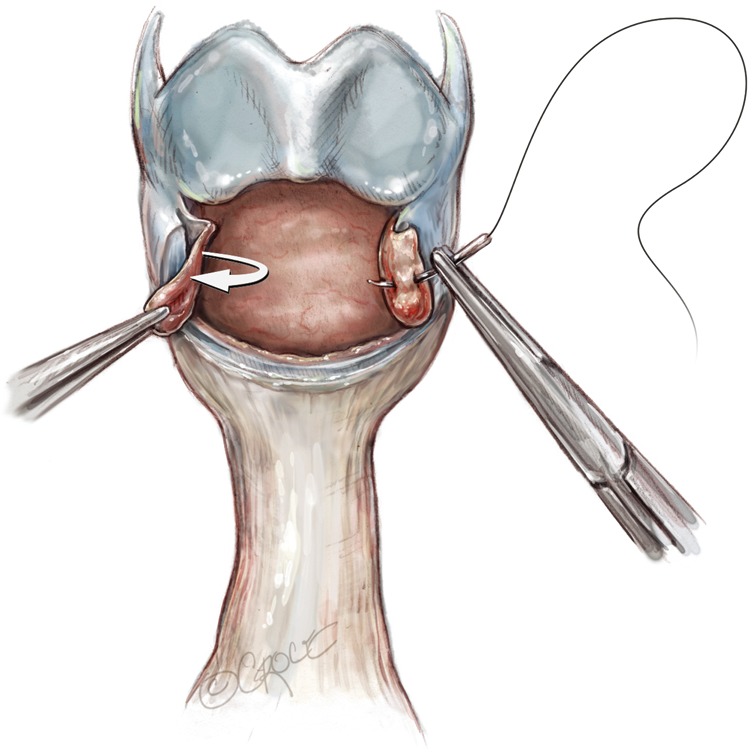
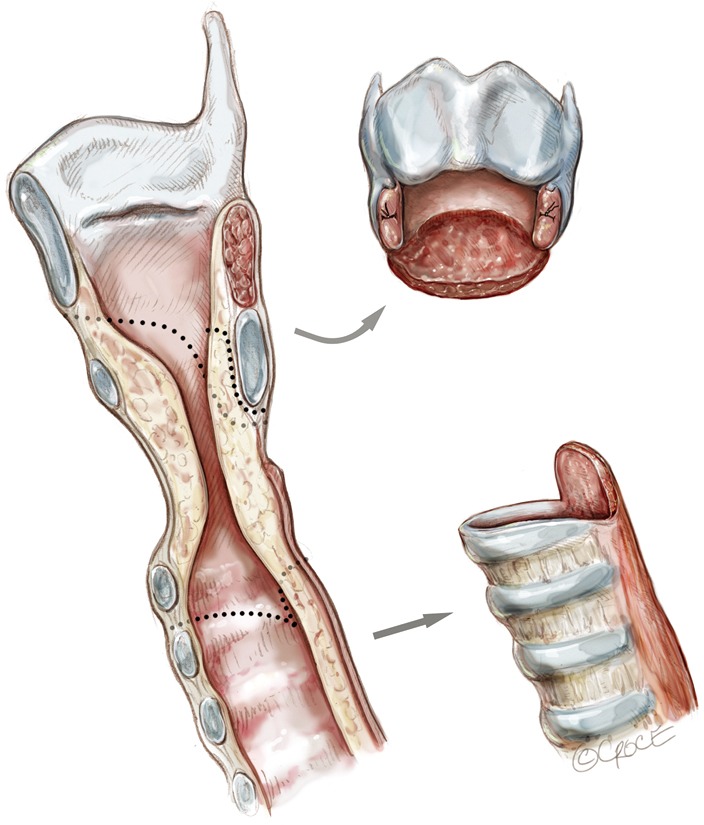
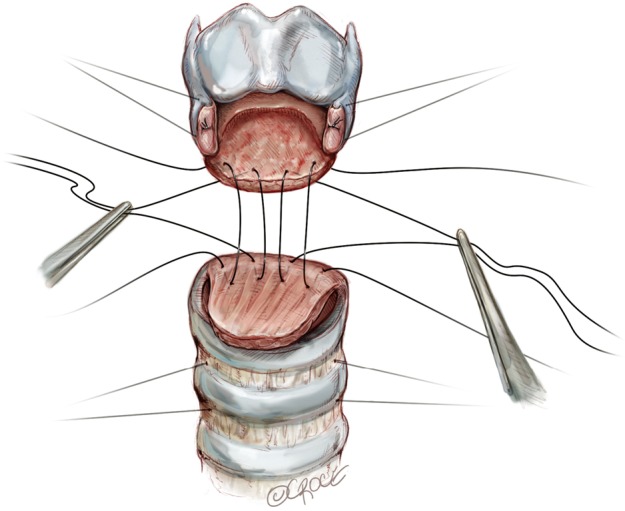
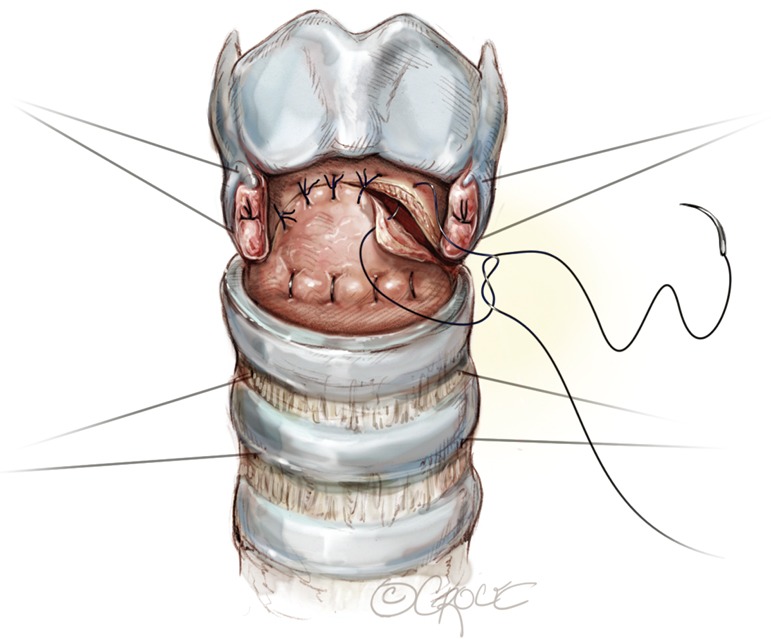
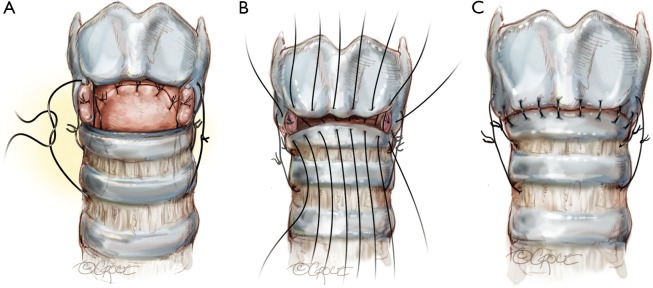
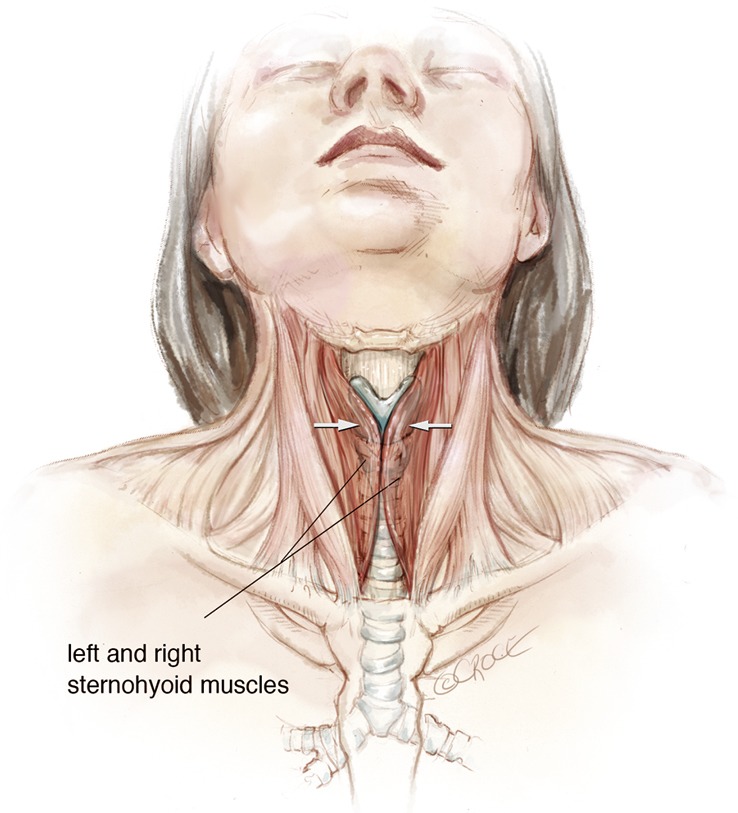
Idiopathic subglottic stenosis is a rare condition of unknown etiology characterized by circumferential stenosis in the subglottic larynx and upper trachea. Historically, patients were treated with dilation or ablation, however this approach has proven to be largely palliative and often leads to recurrence and the need for tracheostomy. A single-staged laryngotracheal resection and reconstruction is now the preferred definitive treatment for idiopathic subglottic stenosis and can be performed with excellent patient outcomes and rare subsequent progression of the disease. Avoiding anastomotic tension and devascularization are important technical keys to minimizing complications.
Keywords: Idiopathic subglottic stenosis; laryngotracheal resection and reconstruction; suprahyoid laryngeal release; tailored cricoplasty.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources