

Minimally invasive anterior, lateral, and oblique lumbar interbody fusion: a literature review
- PMID: 29707553
- PMCID: PMC5900070
- DOI: 10.21037/atm.2018.03.24
Minimally invasive anterior, lateral, and oblique lumbar interbody fusion: a literature review
Abstract
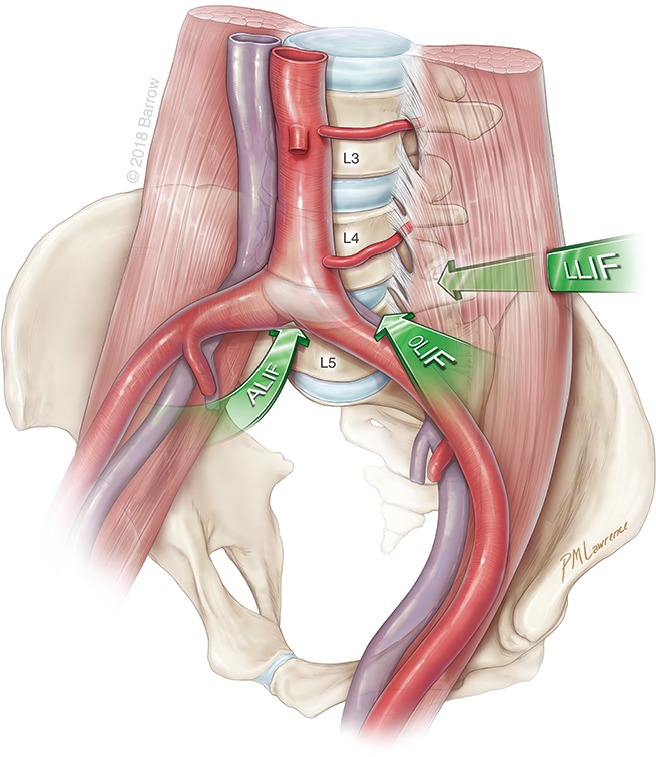
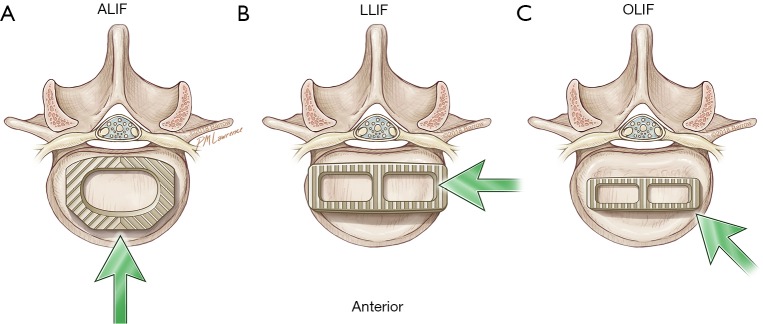
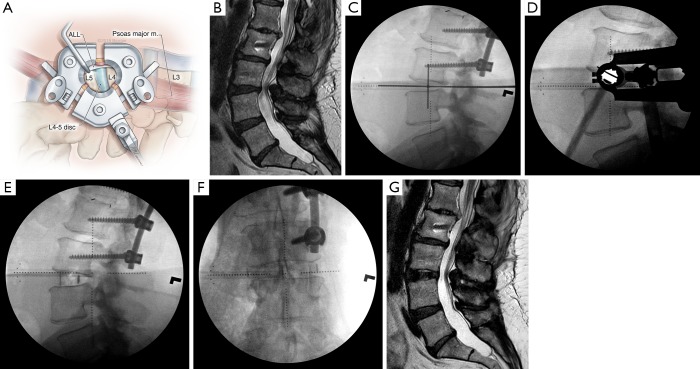
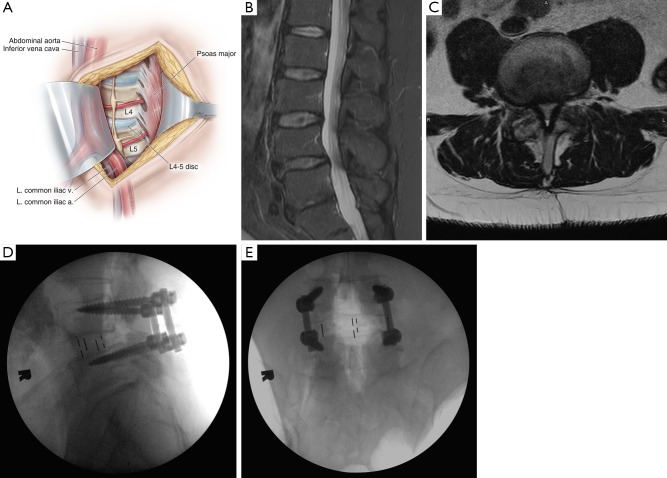
Lumbar interbody fusion involves insertion of a structural graft into an intervertebral disc space to promote bony arthrodesis. It is a well-established surgical strategy for multiple spinal disorders ranging from degenerative conditions to trauma, neoplastic diseases, and deformities requiring correction. Since the inception of lumbar interbody fusion, the most established techniques have been two posterior approaches, the posterior lumbar interbody fusion (PLIF) and the transforaminal lumbar interbody fusion (TLIF). Within the past 15 years, multiple anterolateral approaches to the spine have become widely adopted. These approaches can be performed minimally invasively and spare disruption of the paraspinal muscles and posterior spinal column while enabling wide exposure of the disc space for insertion of interbody grafts much larger than PLIF and TLIF instrumentation. This review highlights three minimally invasive anterolateral approaches: the anterior lumbar interbody fusion (ALIF), the transpsoas lateral lumbar interbody fusion (LLIF), and prepsoas or anterior to the psoas oblique lumbar interbody fusion (OLIF). Relevant topics for discussion and comparison include patient selection, surgical techniques, outcomes, and complications for the three surgical approaches.
Keywords: Anterior lumbar interbody fusion (ALIF); extreme lateral interbody fusion (XLIF); lateral lumbar interbody fusion (LLIF); minimally invasive surgery (MIS); oblique lumbar interbody fusion (OLIF); spinal fusion.
Conflict of interest statement
Conflicts of Interest: Dr. Uribe is a consultant for NuVasive, Inc. The other authors have no conflicts of interest to declare.
Figures
References
-
- Briggs H, Milligan PR. Chip fusion of the low back following exploration of the spinal canal. JBJS 1944;26:125-30.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous