

Simultaneous dual-contrast multi-phase liver imaging using spectral photon-counting computed tomography: a proof-of-concept study
- PMID: 29708205
- PMCID: PMC5909366
- DOI: 10.1186/s41747-017-0030-5
Simultaneous dual-contrast multi-phase liver imaging using spectral photon-counting computed tomography: a proof-of-concept study
Abstract
Background: To assess the feasibility of dual-contrast spectral photon-counting computed tomography (SPCCT) for liver imaging.
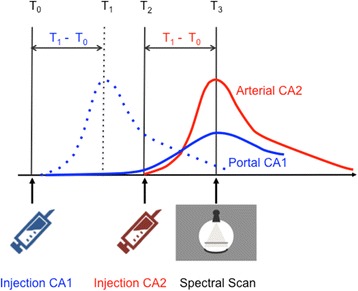
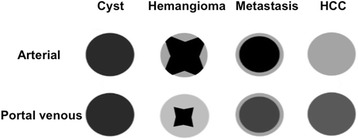
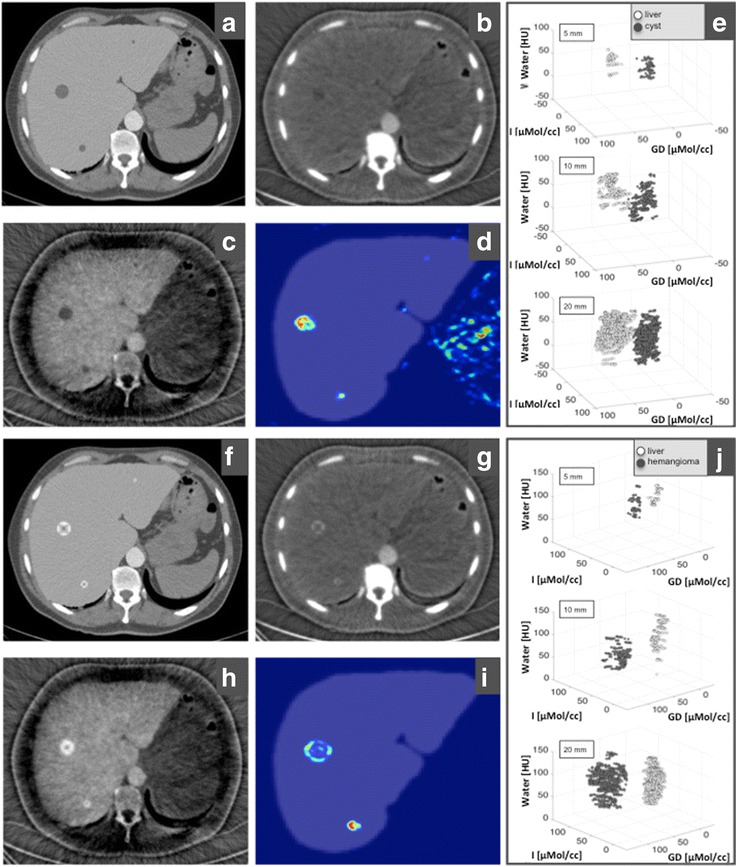
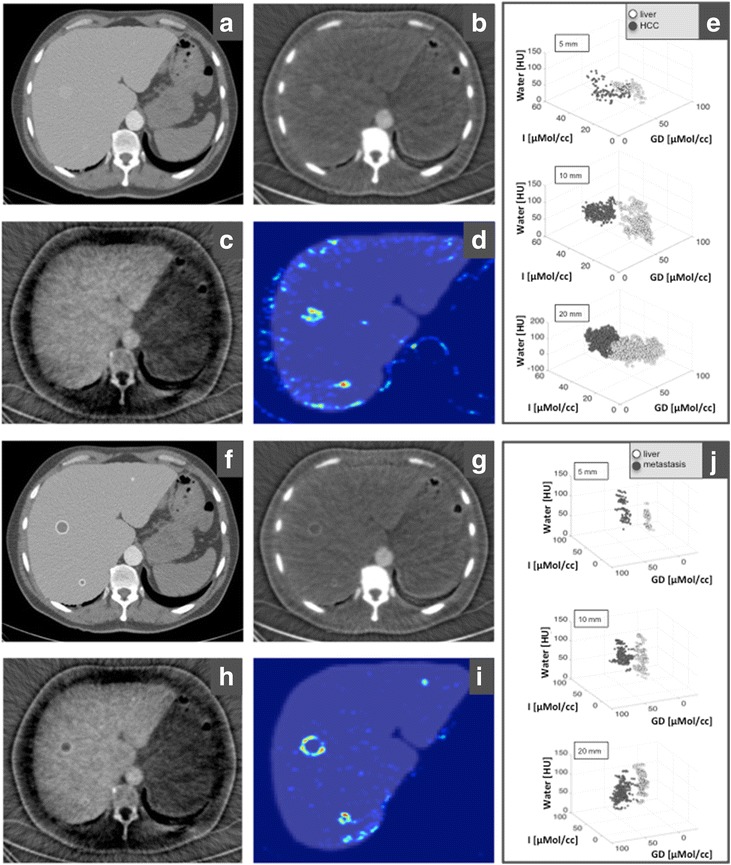
Methods: We present an SPCCT in-silico study for simultaneous mapping of the complementary distribution in the liver of two contrast agents (CAs) subsequently intravenously injected: a gadolinium-based contrast agent and an iodine-based contrast agent. Four types of simulated liver lesions with a characteristic arterial and portal venous pattern (haemangioma, hepatocellular carcinoma, cyst, and metastasis) are presented. A material decomposition was performed to reconstruct quantitative iodine and gadolinium maps. Finally, a multi-dimensional classification algorithm for automatic lesion detection is presented.
Results: Our simulations showed that with a single-scan SPCCT and an adapted contrast injection protocol, it was possible to reconstruct contrast-enhanced images of the liver with arterial distribution of the iodine-based CA and portal venous phase of the gadolinium-based CA. The characteristic patterns of contrast enhancement were visible in all liver lesions. The approach allowed for an automatic detection and classification of liver lesions using a multi-dimensional analysis.
Conclusions: Dual-contrast SPCCT should be able to visualise the characteristic arterial and portal venous enhancement with a single scan, allowing for an automatic lesion detection and characterisation, with a reduced radiation exposure.
Keywords: Computed tomography (CT); Dual-contrast computed tomography; Gadolinium mapping; Gadolinium-based contrast agent; Iodine mapping; Iodine-based contrast agent; Liver; Spectral photon-counting computed tomography (SPCCT).
Conflict of interest statement
HD and RP are employees of Philips Healthcare. The remaining authors (DM, AF, FK, FD, JH, FP, ER and PN) have no financial disclosures and had complete, unrestricted access to the study data at all stages of the study.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Portugaller HR, Stacher R, Komaz G, et al. The value of different spiral CT phases in the detection of liver metastases. Röfo. 2002;174:452–458. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources