

Optical imaging of the breast: evaluation of deoxyhemoglobin concentration alteration in 166 patients with suspicious breast lesions
- PMID: 29708210
- PMCID: PMC5911436
- DOI: 10.1186/s41747-018-0038-5
Optical imaging of the breast: evaluation of deoxyhemoglobin concentration alteration in 166 patients with suspicious breast lesions
Abstract
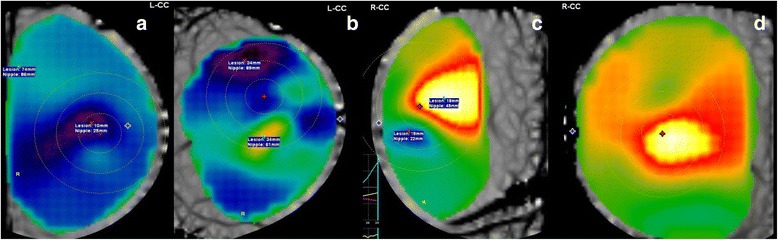
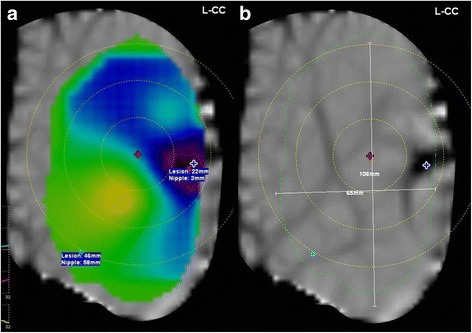
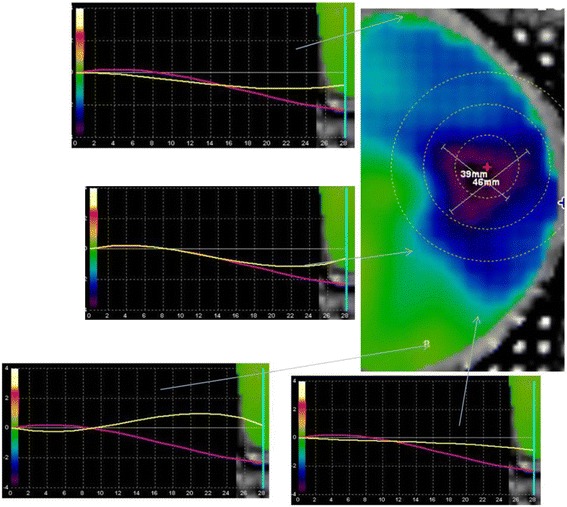
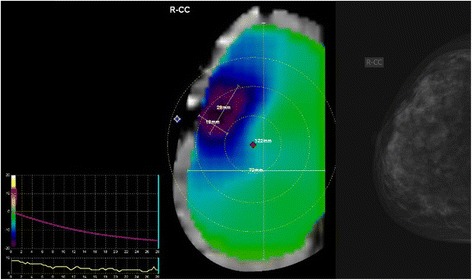
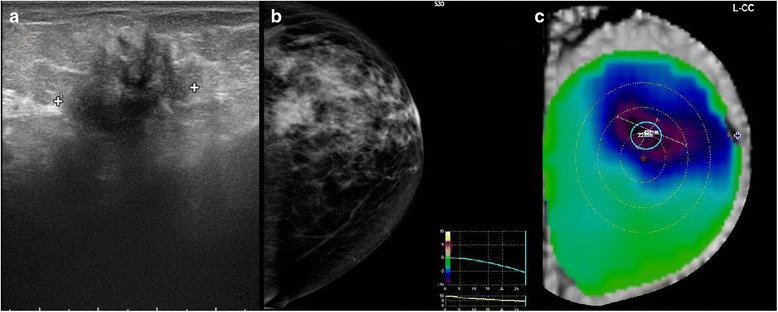
Background: We investigated the performance of optical imaging evaluating deoxyhemoglobin concentration alteration (DeHCA) in breast tissues.
Methods: We enrolled all consecutive patients from January 2015 to October 2016 with clinically suspicious and/or BI-RADS grade 3-5 lesions at mammography or ultrasound (US). Patients underwent optical imaging (ComfortScan) to evaluate for DeHCA. The reference standard was pathology from a surgical specimen for malignant lesions, pathology from a surgical specimen or core needle biopsy for benign lesions, and negative follow-up for contralateral negative breasts. Non-parametric statistics, receiver operating characteristic, and linear discrimination analyses were performed.
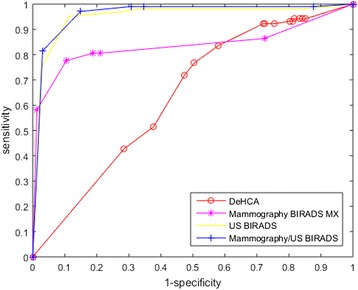
Results: Of 334 enrolled patients, 168 (50%) were excluded for technical problems and 166 (50%) (median age 52 years) were analyzed totaling 331 breasts and 176 lesions. Of these, 75 were benign (median size 19 mm) and 101 malignant (median size 20 mm). The median DeHCA score in malignant lesions (0.95, interquartile range [IQR] 1.00-0.87) was higher (p < 0.001) than in benign lesions (0.80, IQR 0.95-0.70). Using the optimal cutoff (0.85), DeHCA score was less accurate than mammography, US, and their combination, with 78% sensitivity, 52% specificity, 40% positive predictive value (PPV), and 85% negative predictive value (NPV); using a 0.8 cutoff, sensitivity reached 93% and NPV 91%, but specificity fell to 32% and PPV to 37%. The accuracy of DeHCA score linearly combined with mammography or US was higher than that of DeHCA score alone (p < 0.001) and not significantly higher than that of mammography or US alone.
Conclusions: DeHCA score was significantly higher in malignant than in benign lesions, but its accuracy was significantly lower than that of mammography or US. Future refinements are needed.
Keywords: Breast cancer; Breast ultrasound; Deoxyhemoglobin concentration alteration; Mammography; Optical imaging.
Conflict of interest statement
This study was performed according to regulations issued by our local Institutional Review Board.All patients provided informed consent for the use of their data for research purposes.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures








Similar articles
-
Supplemental use of optical diffusion breast imaging for differentiation between benign and malignant breast lesions.AJR Am J Roentgenol. 2011 Sep;197(3):732-9. doi: 10.2214/AJR.10.5102. AJR Am J Roentgenol. 2011. PMID: 21862818
-
Contrast-enhanced MR imaging in patients with BI-RADS 3-5 microcalcifications.Radiol Med. 2007 Mar;112(2):272-86. doi: 10.1007/s11547-007-0141-9. Epub 2007 Mar 19. Radiol Med. 2007. PMID: 17361370 English, Italian.
-
Role of combined BI-RADS assessment using mammography and sonography for evaluation of incidental hypermetabolic lesions in the breast on 18F-FDG PET-CT.Acta Radiol. 2013 Dec;54(10):1117-24. doi: 10.1177/0284185113492453. Epub 2013 Jul 17. Acta Radiol. 2013. PMID: 23864064
-
Validity of breast-specific gamma imaging for Breast Imaging Reporting and Data System 4 lesions on mammography and/or ultrasound.Ann Surg Treat Res. 2016 Apr;90(4):194-200. doi: 10.4174/astr.2016.90.4.194. Epub 2016 Mar 30. Ann Surg Treat Res. 2016. PMID: 27073789 Free PMC article.
-
The negative predictive value of electrical impedance scanning in BI-RADS category IV breast lesions.Invest Radiol. 2005 Jul;40(7):478-85. doi: 10.1097/01.rli.0000167425.34577.d1. Invest Radiol. 2005. PMID: 15973141
Cited by
-
Recent Advances in Ultrasound Breast Imaging: From Industry to Clinical Practice.Diagnostics (Basel). 2023 Mar 4;13(5):980. doi: 10.3390/diagnostics13050980. Diagnostics (Basel). 2023. PMID: 36900124 Free PMC article. Review.
-
Introduction to Special Issue of Radiology and Imaging of Cancer.Cancers (Basel). 2020 Sep 18;12(9):2665. doi: 10.3390/cancers12092665. Cancers (Basel). 2020. PMID: 32961946 Free PMC article.
-
Intelligent scoring system based on dynamic optical breast imaging for early detection of breast cancer.Biomed Opt Express. 2024 Feb 9;15(3):1515-1527. doi: 10.1364/BOE.515135. eCollection 2024 Mar 1. Biomed Opt Express. 2024. PMID: 38495695 Free PMC article.
-
Detection of breast cancer using machine learning on time-series diffuse optical transillumination data.J Biomed Opt. 2024 Nov;29(11):115001. doi: 10.1117/1.JBO.29.11.115001. Epub 2024 Nov 11. J Biomed Opt. 2024. PMID: 39529875 Free PMC article.
References
-
- Breast Cancer Estimated Incidence, Mortality and Prevalence Worldwide in 2012 (2012). http://ww5.komen.org/BreastCancer/Statistics.html. Accessed 21 Mar 2017.
LinkOut - more resources
Full Text Sources
Other Literature Sources