

Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer
- PMID: 29708592
- PMCID: PMC6033157
- DOI: 10.1002/bjs.10870
Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer
Abstract
Background: Studies comparing upfront surgery with neoadjuvant treatment in pancreatic cancer may report only patients who underwent resection and so survival will be skewed. The aim of this study was to report survival by intention to treat in a comparison of upfront surgery versus neoadjuvant treatment in resectable or borderline resectable pancreatic cancer.
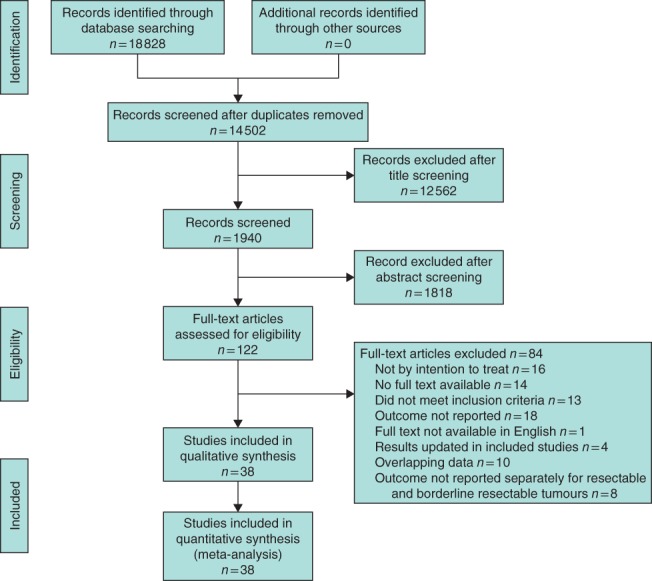
Methods: MEDLINE, Embase and the Cochrane Library were searched for studies reporting median overall survival by intention to treat in patients with resectable or borderline resectable pancreatic cancer treated with or without neoadjuvant treatment. Secondary outcomes included overall and R0 resection rate, pathological lymph node rate, reasons for unresectability and toxicity of neoadjuvant treatment.
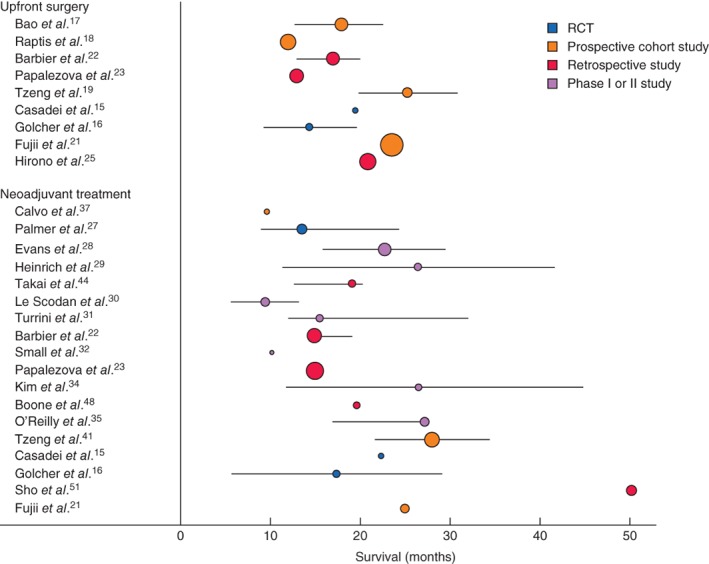
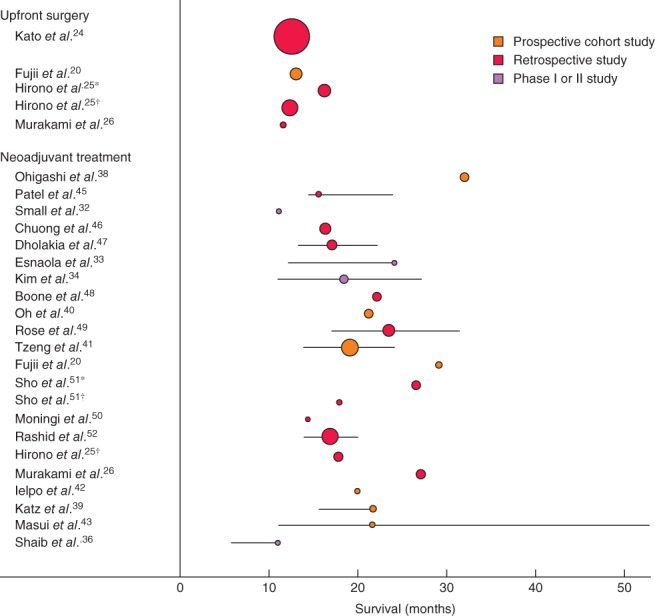
Results: In total, 38 studies were included with 3484 patients, of whom 1738 (49·9 per cent) had neoadjuvant treatment. The weighted median overall survival by intention to treat was 18·8 months for neoadjuvant treatment and 14·8 months for upfront surgery; the difference was larger among patients whose tumours were resected (26·1 versus 15·0 months respectively). The overall resection rate was lower with neoadjuvant treatment than with upfront surgery (66·0 versus 81·3 per cent; P < 0·001), but the R0 rate was higher (86·8 (95 per cent c.i. 84·6 to 88·7) versus 66·9 (64·2 to 69·6) per cent; P < 0·001). Reported by intention to treat, the R0 rates were 58·0 and 54·9 per cent respectively (P = 0·088). The pathological lymph node rate was 43·8 per cent after neoadjuvant therapy and 64·8 per cent in the upfront surgery group (P < 0·001). Toxicity of at least grade III was reported in up to 64 per cent of the patients.
Conclusion: Neoadjuvant treatment appears to improve overall survival by intention to treat, despite lower overall resection rates for resectable or borderline resectable pancreatic cancer. PROSPERO registration number: CRD42016049374.
© 2018 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Neoptolemos JP, Palmer DH, Ghaneh P, Psarelli EE, Valle JW, Halloran CM et al; European Study Group for Pancreatic Cancer. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC‐4): a multicentre, open‐label, randomised, phase 3 trial. Lancet 2017; 389: 1011–1024. - PubMed
-
- Sinn M, Bahra M, Liersch T, Gellert K, Messmann H, Bechstein W et al CONKO‐005: adjuvant chemotherapy with gemcitabine plus erlotinib versus gemcitabine alone in patients after R0 resection of pancreatic cancer: a multicenter randomized phase III trial. J Clin Oncol 2017; 35: 3330–3337. - PubMed
-
- Shaib Y, Davila J, Naumann C, El‐Serag H. The impact of curative intent surgery on the survival of pancreatic cancer patients: a U.S. population‐based study. Am J Gastroenterol 2007; 102: 1377–1382. - PubMed
-
- Stessin AM, Meyer JE, Sherr DL. Neoadjuvant radiation is associated with improved survival in patients with resectable pancreatic cancer: an analysis of data from the surveillance, epidemiology, and end results (SEER) registry. Int J Radiat Oncol Biol Phys 2008; 72: 1128–1133. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
