

Microdeletion on chromosome 8p23.1 in a familial form of severe Buruli ulcer
- PMID: 29708969
- PMCID: PMC5945055
- DOI: 10.1371/journal.pntd.0006429
Microdeletion on chromosome 8p23.1 in a familial form of severe Buruli ulcer
Abstract
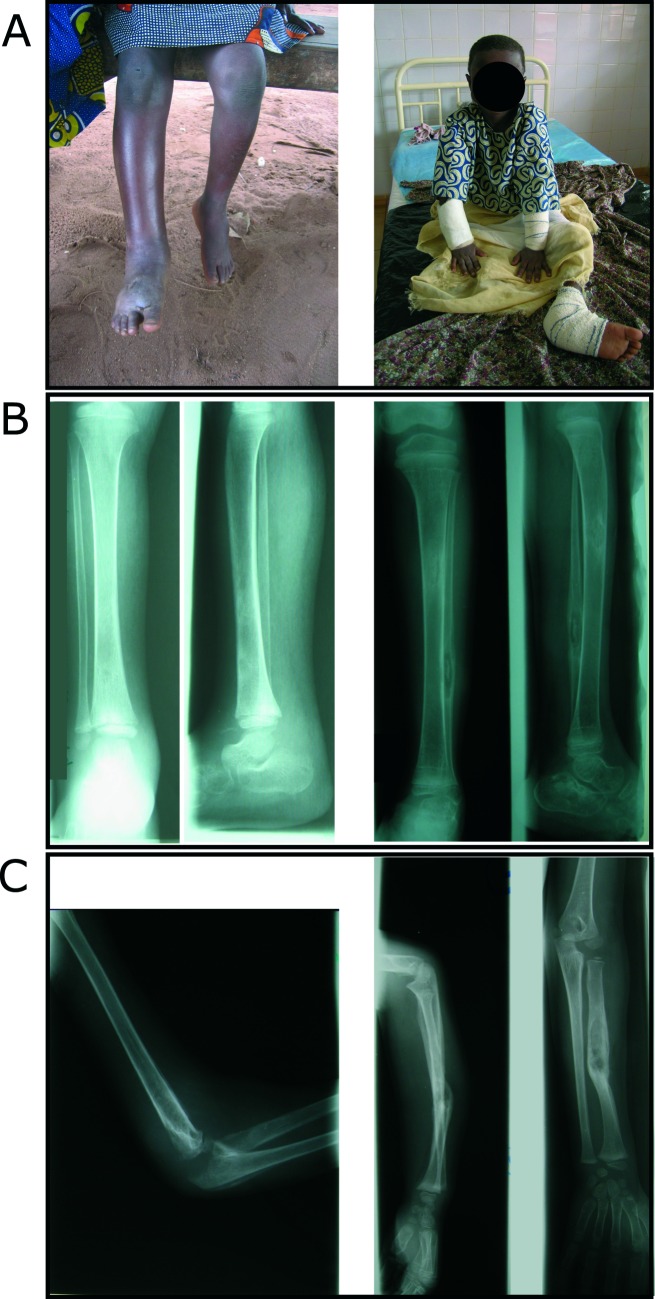
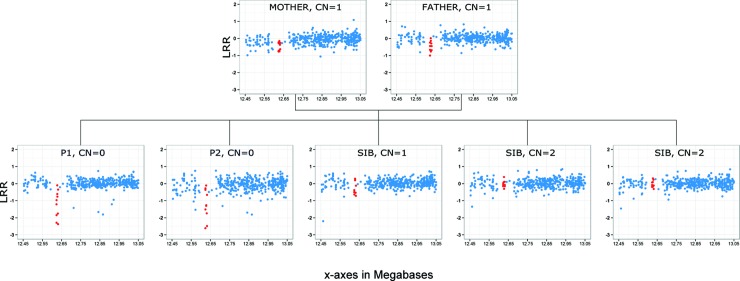
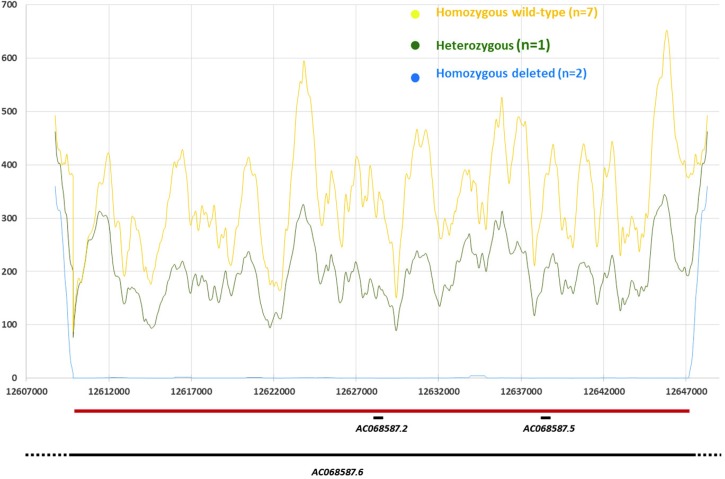
Buruli ulcer (BU), the third most frequent mycobacteriosis worldwide, is a neglected tropical disease caused by Mycobacterium ulcerans. We report the clinical description and extensive genetic analysis of a consanguineous family from Benin comprising two cases of unusually severe non-ulcerative BU. The index case was the most severe of over 2,000 BU cases treated at the Centre de Dépistage et de Traitement de la Lèpre et de l'Ulcère de Buruli, Pobe, Benin, since its opening in 2003. The infection spread to all limbs with PCR-confirmed skin, bone and joint infections. Genome-wide linkage analysis of seven family members was performed and whole-exome sequencing of both patients was obtained. A 37 kilobases homozygous deletion confirmed by targeted resequencing and located within a linkage region on chromosome 8 was identified in both patients but was absent from unaffected siblings. We further assessed the presence of this deletion on genotyping data from 803 independent local individuals (402 BU cases and 401 BU-free controls). Two BU cases were predicted to be homozygous carriers while none was identified in the control group. The deleted region is located close to a cluster of beta-defensin coding genes and contains a long non-coding (linc) RNA gene previously shown to display highest expression values in the skin. This first report of a microdeletion co-segregating with severe BU in a large family supports the view of a key role of human genetics in the natural history of the disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Sizaire V, Nackers F, Comte E, Portaels F. Mycobacterium ulcerans infection: control, diagnosis, and treatment. Lancet Infect Dis. 2006;6(5):288–96. Epub 2006/04/25. S1473-3099(06)70464-9 [pii] doi: 10.1016/S1473-3099(06)70464-9 . - DOI - PubMed
-
- World Health Organization. Buruli ulcer disease factsheet 2017. Available from: http://www.who.int/mediacentre/factsheets/fs199/en/index.html
-
- Eddyani M, Sopoh GE, Ayelo G, Brun LVC, Roux JJ, Barogui Y, et al. Diagnostic Accuracy of Clinical and Microbiological Signs in Patients with Skin Lesions Resembling Buruli Ulcer in an Endemic Region. Clin Infect Dis. 2018. doi: 10.1093/cid/ciy197 . - DOI - PMC - PubMed
-
- Vincent QB, Ardant MF, Adeye A, Goundote A, Saint-Andre JP, Cottin J, et al. Clinical epidemiology of laboratory-confirmed Buruli ulcer in Benin: a cohort study. Lancet Glob Health. 2014;2(7):e422–30. Epub 2014/08/12. S2214-109X(14)70223-2 [pii] doi: 10.1016/S2214-109X(14)70223-2 . - DOI - PubMed
-
- Vincent QB, Ardant MF, Marsollier L, Chauty A, Alcais A. HIV infection and Buruli ulcer in Africa. Lancet Infect Dis. 2014;14(9):796–7. Epub 2014/08/29. S1473-3099(14)70882-5 [pii] doi: 10.1016/S1473-3099(14)70882-5 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
