

Biological exacerbation clusters demonstrate asthma and chronic obstructive pulmonary disease overlap with distinct mediator and microbiome profiles
- PMID: 29709671
- PMCID: PMC5986707
- DOI: 10.1016/j.jaci.2018.04.013
Biological exacerbation clusters demonstrate asthma and chronic obstructive pulmonary disease overlap with distinct mediator and microbiome profiles
Abstract
Background: Exacerbations of asthma and chronic obstructive pulmonary disease (COPD) are heterogeneous.
Objective: We sought to investigate the sputum cellular, mediator, and microbiome profiles of both asthma and COPD exacerbations.
Methods: Patients with severe asthma or moderate-to-severe COPD were recruited prospectively to a single center. Sputum mediators were available in 32 asthmatic patients and 73 patients with COPD assessed at exacerbation. Biologic clusters were determined by using factor and cluster analyses on a panel of sputum mediators. Patterns of clinical parameters, sputum mediators, and microbiome communities were assessed across the identified clusters.
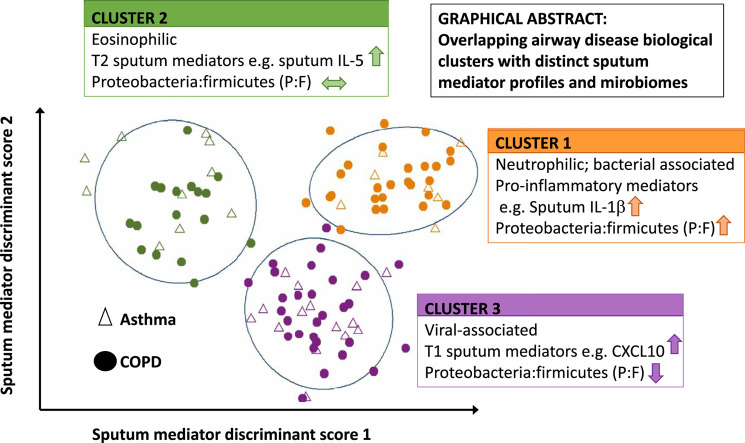
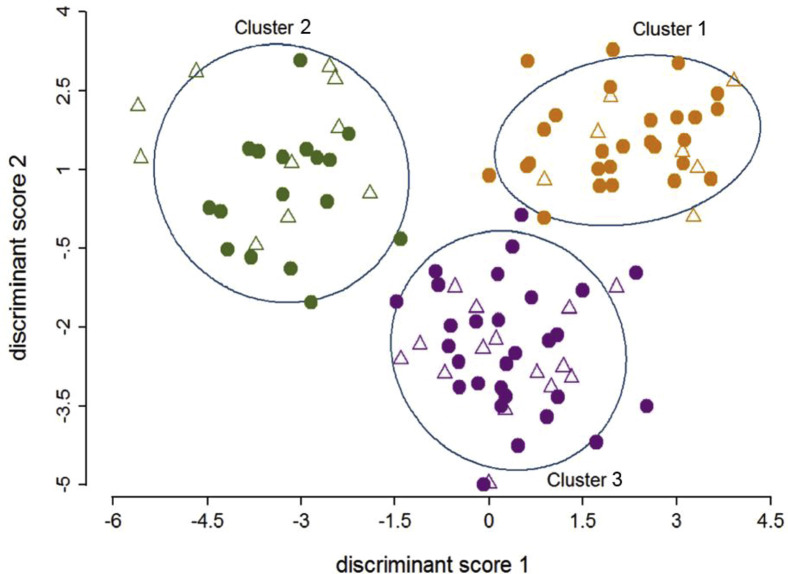
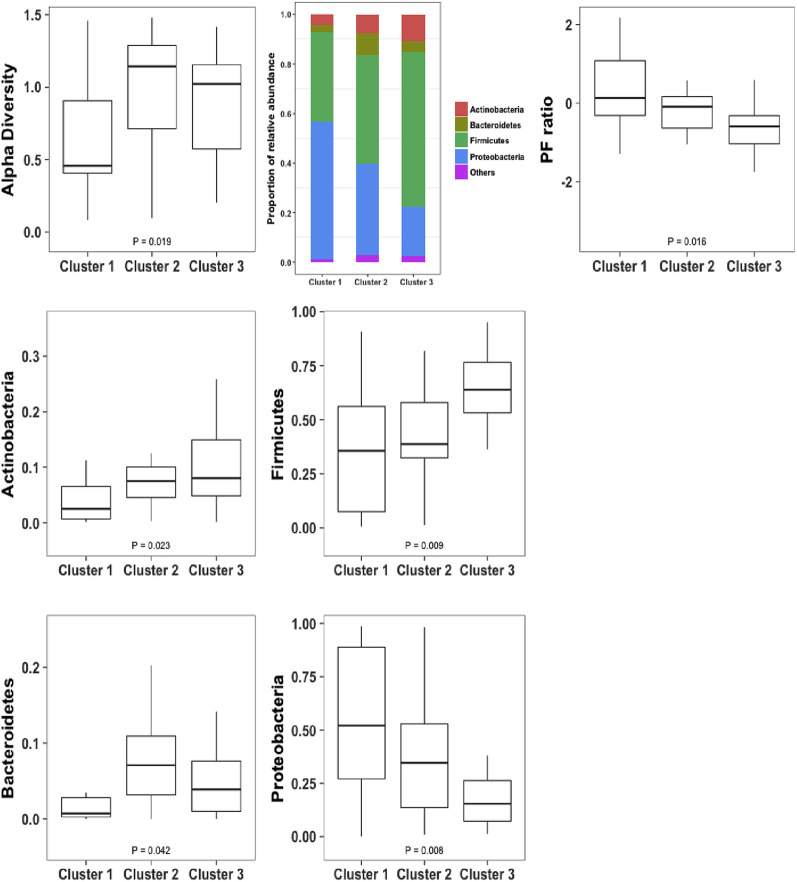
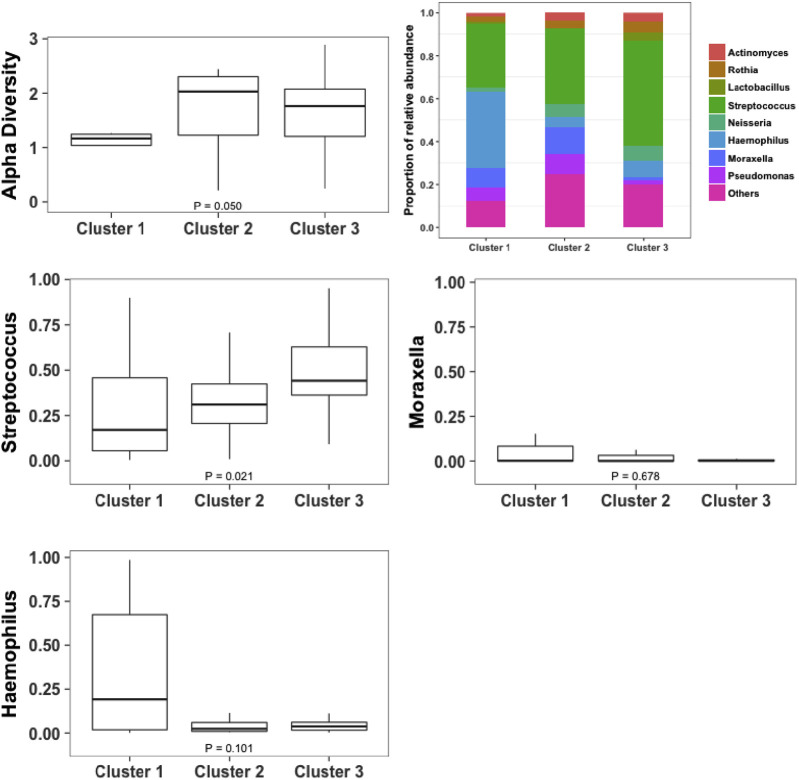
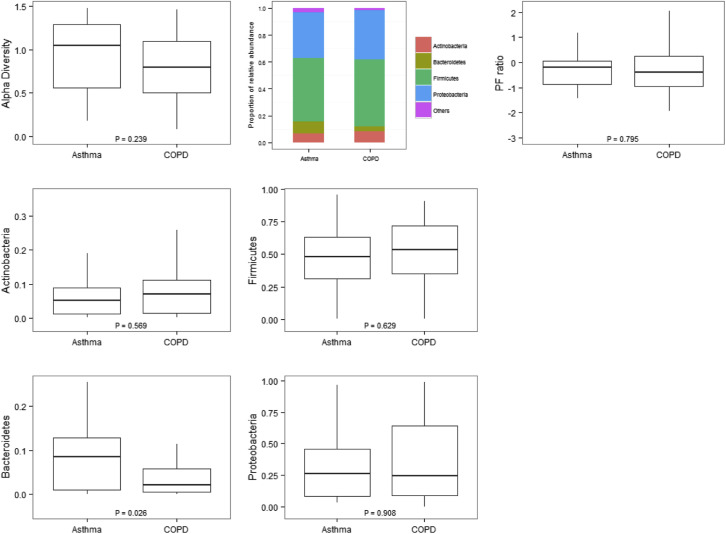
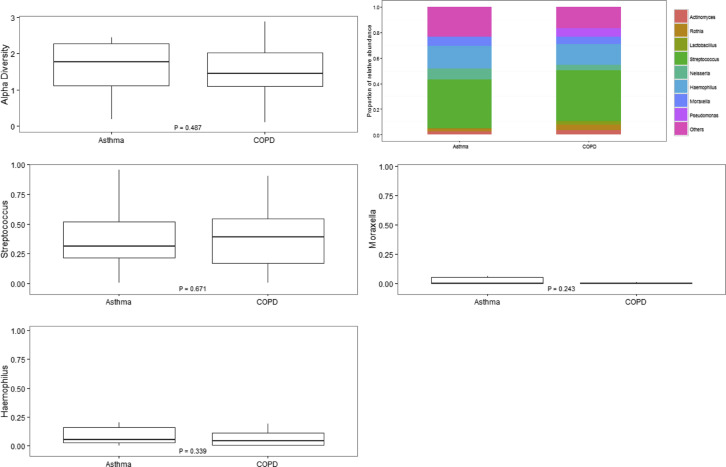
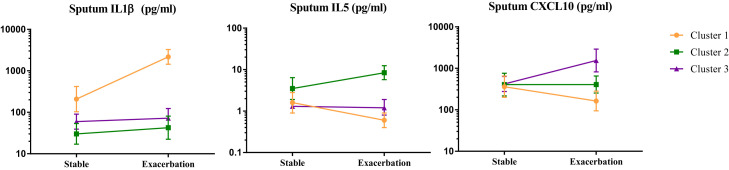
Results: The asthmatic patients and patients with COPD had different clinical characteristics and inflammatory profiles but similar microbial ecology. Three exacerbation biologic clusters were identified. Cluster 1 was COPD predominant, with 27 patients with COPD and 7 asthmatic patients exhibiting increased blood and sputum neutrophil counts, proinflammatory mediators (IL-1β, IL-6, IL-6 receptor, TNF-α, TNF receptors 1 and 2, and vascular endothelial growth factor), and proportions of the bacterial phylum Proteobacteria. Cluster 2 had 10 asthmatic patients and 17 patients with COPD with increased blood and sputum eosinophil counts, type 2 mediators (IL-5, IL-13, CCL13, CCL17, and CCL26), and proportions of the bacterial phylum Bacteroidetes. Cluster 3 had 15 asthmatic patients and 29 patients with COPD with increased type 1 mediators (CXCL10, CXCL11, and IFN-γ) and proportions of the phyla Actinobacteria and Firmicutes.
Conclusions: A biologic clustering approach revealed 3 subgroups of asthma and COPD exacerbations, each with different percentages of patients with overlapping asthma and COPD. The sputum mediator and microbiome profiles were distinct between clusters.
Keywords: Asthma; asthma and chronic obstructive pulmonary disease heterogeneity; chronic obstructive pulmonary disease; factor and cluster analyses; inflammatory profiles; microbiome abundances; phylum and genus levels.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388:1545–1602. - PMC - PubMed
-
- Bafadhel M., McKenna S., Terry S., Mistry V., Reid C., Haldar P. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184:662–671. - PubMed
-
- Siroux V., Basagana X., Boudier A., Pin I., Garcia-Aymerich J., Vesin A. Identifying adult asthma phenotypes using a clustering approach. Eur Respir J. 2011;38:310–317. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
