

Association of Prehospital Advanced Life Support by Physician With Survival After Out-of-Hospital Cardiac Arrest With Blunt Trauma Following Traffic Collisions: Japanese Registry-Based Study
- PMID: 29710068
- PMCID: PMC6145650
- DOI: 10.1001/jamasurg.2018.0674
Association of Prehospital Advanced Life Support by Physician With Survival After Out-of-Hospital Cardiac Arrest With Blunt Trauma Following Traffic Collisions: Japanese Registry-Based Study
Abstract
Importance: Controversy remains as to whether advanced life support (ALS) or basic life support (BLS) is superior for critically ill and injured patients, including out-of-hospital cardiac arrest (OHCA) and major trauma, in the prehospital setting.
Objective: To assess whether prehospital ALS should be provided for traumatic OHCA and who should perform it.
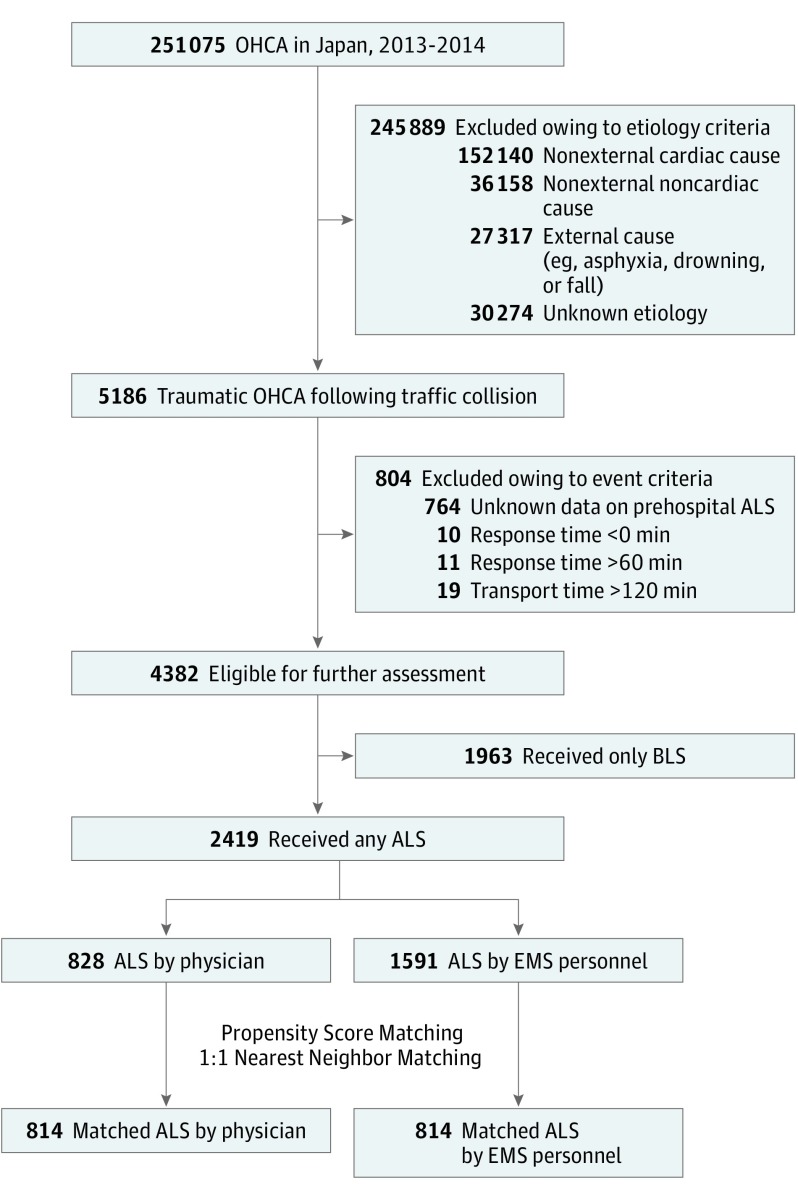
Design, setting, and participants: Japanese government-managed nationwide population-based registry data of patients with OHCA transported to an emergency hospital were analyzed. Patients who experienced traumatic OHCA following a traffic collision from 2013 to 2014 were included. Patients provided prehospital ALS by a physician were compared with both patients provided ALS by emergency medical service (EMS) personnel and patients with only BLS. The data were analyzed on May 1, 2017.
Exposures: Advanced life support by physician, ALS by EMS personnel, or BLS only.
Main outcomes and measures: The primary outcome was 1-month survival. The secondary outcomes were prehospital return of spontaneous circulation and favorable neurologic outcomes with the Glasgow-Pittsburgh cerebral performance category score of 1 or 2.
Results: A total of 4382 patients were included (mean [SD] age, 57.5 [22.2] years; 67.9% male); 828 (18.9%) received prehospital ALS by physician, 1591 (36.3%) received prehospital ALS by EMS personnel, and 1963 (44.8%) received BLS only. Among these patients, 96 (2.2%) survived 1 month after OHCA, including 26 of 828 (3.1%) for ALS by physician, 25 of 1591 (1.6%) for ALS by EMS personnel, and 45 of 1963 (2.3%) for BLS. After adjusting for potential confounders using multivariable logistic regression, ALS by physician was significantly associated with higher odds for 1-month survival compared with both ALS by EMS personnel and BLS (adjusted OR, 2.13; 95% CI, 1.20-3.78; and adjusted OR, 1.94; 95% CI, 1.14-3.25; respectively), whereas there was no significant difference between ALS by EMS personnel and BLS (adjusted OR, 0.91; 95% CI, 0.54-1.51). A propensity score-matched analysis in the ALS cohort showed that ALS by physician was associated with increased chance of 1-month survival compared with ALS by EMS personnel (risk ratio, 2.00; 95% CI, 1.01-3.97; P = .04). This association was consistent across a variety of sensitivity analyses.
Conclusions and relevance: In traumatic OHCA, ALS by physician was associated with increased chance of 1-month survival compared with both ALS by EMS personnel and BLS.
Conflict of interest statement
Figures
Comment in
-
In Blunt Traumatic Cardiac Arrest, Does It Really Matter Who Performs Prehospital Advanced Life Support?JAMA Surg. 2018 Jun 20;153(6):e180675. doi: 10.1001/jamasurg.2018.0675. Epub 2018 Jun 20. JAMA Surg. 2018. PMID: 29710131 No abstract available.
-
Prehospital Advanced Life Support for Out-of-Hospital Cardiac Arrest in Blunt Trauma Patients.JAMA Surg. 2019 Jan 1;154(1):95-96. doi: 10.1001/jamasurg.2018.4291. JAMA Surg. 2019. PMID: 30422252 No abstract available.
Similar articles
-
Impact of prehospital physician-led cardiopulmonary resuscitation on neurologically intact survival after out-of-hospital cardiac arrest: A nationwide population-based observational study.Resuscitation. 2019 Mar;136:38-46. doi: 10.1016/j.resuscitation.2018.11.014. Epub 2018 Nov 15. Resuscitation. 2019. PMID: 30448503
-
Advanced vs. Basic Life Support in the Treatment of Out-of-Hospital Cardiopulmonary Arrest in the Resuscitation Outcomes Consortium.Resuscitation. 2018 Jul;128:132-137. doi: 10.1016/j.resuscitation.2018.04.031. Epub 2018 Apr 30. Resuscitation. 2018. PMID: 29723609
-
Prehospital epinephrine use and survival among patients with out-of-hospital cardiac arrest.JAMA. 2012 Mar 21;307(11):1161-8. doi: 10.1001/jama.2012.294. JAMA. 2012. PMID: 22436956
-
When is a Cardiac Arrest Non-Cardiac?Prehosp Disaster Med. 2017 Oct;32(5):523-527. doi: 10.1017/S1049023X17006446. Epub 2017 May 2. Prehosp Disaster Med. 2017. PMID: 28463098 Review.
-
Prehospital Physician Presence for Patients With out-of-Hospital Cardiac Arrest Undergoing Extracorporeal Cardiopulmonary Resuscitation: A Multicenter, Retrospective, Nationwide Observational Study in Japan (The JAAM-OHCA registry).Curr Probl Cardiol. 2023 May;48(5):101600. doi: 10.1016/j.cpcardiol.2023.101600. Epub 2023 Jan 18. Curr Probl Cardiol. 2023. PMID: 36681207 Review.
Cited by
-
Resuscitative endovascular balloon occlusion of the aorta and traumatic out-of-hospital cardiac arrest: A nationwide study.J Am Coll Emerg Physicians Open. 2020 Jul 4;1(4):624-632. doi: 10.1002/emp2.12177. eCollection 2020 Aug. J Am Coll Emerg Physicians Open. 2020. PMID: 33000081 Free PMC article.
-
Prehospital advanced airway management of emergency medical service-witnessed traumatic out-of-hospital cardiac arrest patients: analysis of nationwide trauma registry.Acute Med Surg. 2022 Sep 16;9(1):e786. doi: 10.1002/ams2.786. eCollection 2022 Jan-Dec. Acute Med Surg. 2022. PMID: 36176323 Free PMC article.
-
Benefits of targeted deployment of physician-led interprofessional pre-hospital teams on the care of critically Ill and injured patients: a systematic review and meta-analysis.Scand J Trauma Resusc Emerg Med. 2025 Jan 6;33(1):1. doi: 10.1186/s13049-024-01298-8. Scand J Trauma Resusc Emerg Med. 2025. PMID: 39757222 Free PMC article.
-
Association of Prehospital Epinephrine Administration With Survival Among Patients With Traumatic Cardiac Arrest Caused By Traffic Collisions.Sci Rep. 2019 Jul 9;9(1):9922. doi: 10.1038/s41598-019-46460-w. Sci Rep. 2019. PMID: 31289342 Free PMC article.
-
Effects of physician-present prehospital care in patients with out-of-hospital cardiac arrest on return of spontaneous circulation: A retrospective, observational study in Saga, Japan.Health Sci Rep. 2024 Apr 22;7(4):e1981. doi: 10.1002/hsr2.1981. eCollection 2024 Apr. Health Sci Rep. 2024. PMID: 38655425 Free PMC article.
References
-
- Kitamura T, Iwami T, Kawamura T, et al. ; Japanese Circulation Society Resuscitation Science Study Group . Nationwide improvements in survival from out-of-hospital cardiac arrest in Japan. Circulation. 2012;126(24):-. - PubMed
-
- Nakahara S, Tomio J, Ichikawa M, et al. . Association of bystander intervenetions with neurologically intact survival among patients with bystander-witnessed out-of-hospital cardiac arrest in Japan. JAMA. 2015;314(3):247-254. - PubMed
-
- Tsutsumi Y, Fukuma S, Tsuchiya A, et al. . Association between spinal immobilization and survival at discharge for on-scene blunt traumatic cardiac arrest: a nationwide retrospective cohort study. Injury. 2018;49(1):124-129. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
