

Exercise Early and Often: Effects of Physical Activity and Exercise on Women's Bone Health
- PMID: 29710770
- PMCID: PMC5981917
- DOI: 10.3390/ijerph15050878
Exercise Early and Often: Effects of Physical Activity and Exercise on Women's Bone Health
Abstract
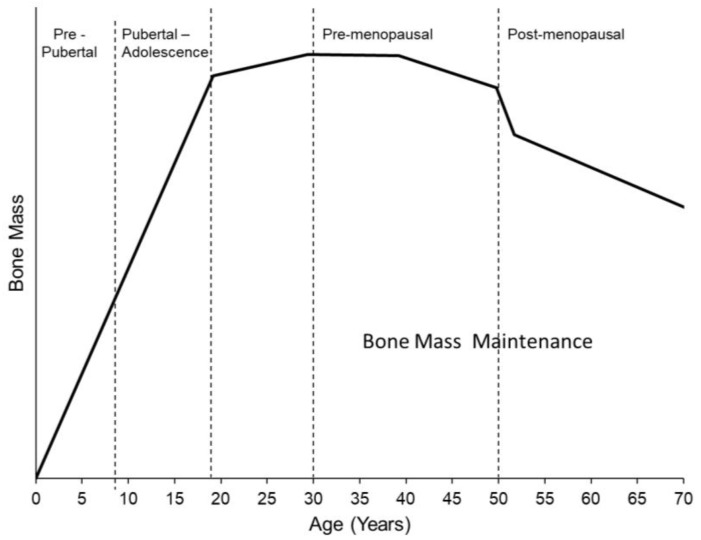
In 2011 over 1.7 million people were hospitalized because of a fragility fracture, and direct costs associated with osteoporosis treatment exceeded 70 billion dollars in the United States. Failure to reach and maintain optimal peak bone mass during adulthood is a critical factor in determining fragility fracture risk later in life. Physical activity is a widely accessible, low cost, and highly modifiable contributor to bone health. Exercise is especially effective during adolescence, a time period when nearly 50% of peak adult bone mass is gained. Here, we review the evidence linking exercise and physical activity to bone health in women. Bone structure and quality will be discussed, especially in the context of clinical diagnosis of osteoporosis. We review the mechanisms governing bone metabolism in the context of physical activity and exercise. Questions such as, when during life is exercise most effective, and what specific types of exercises improve bone health, are addressed. Finally, we discuss some emerging areas of research on this topic, and summarize areas of need and opportunity.
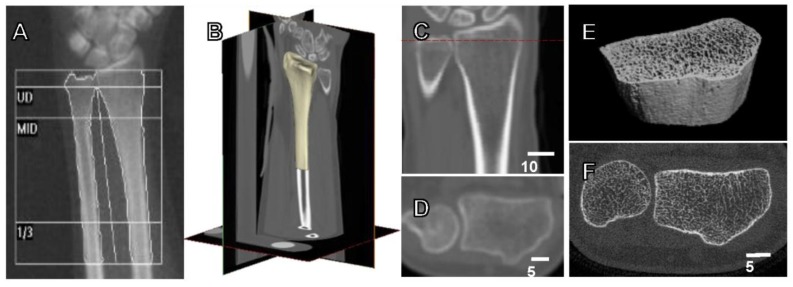
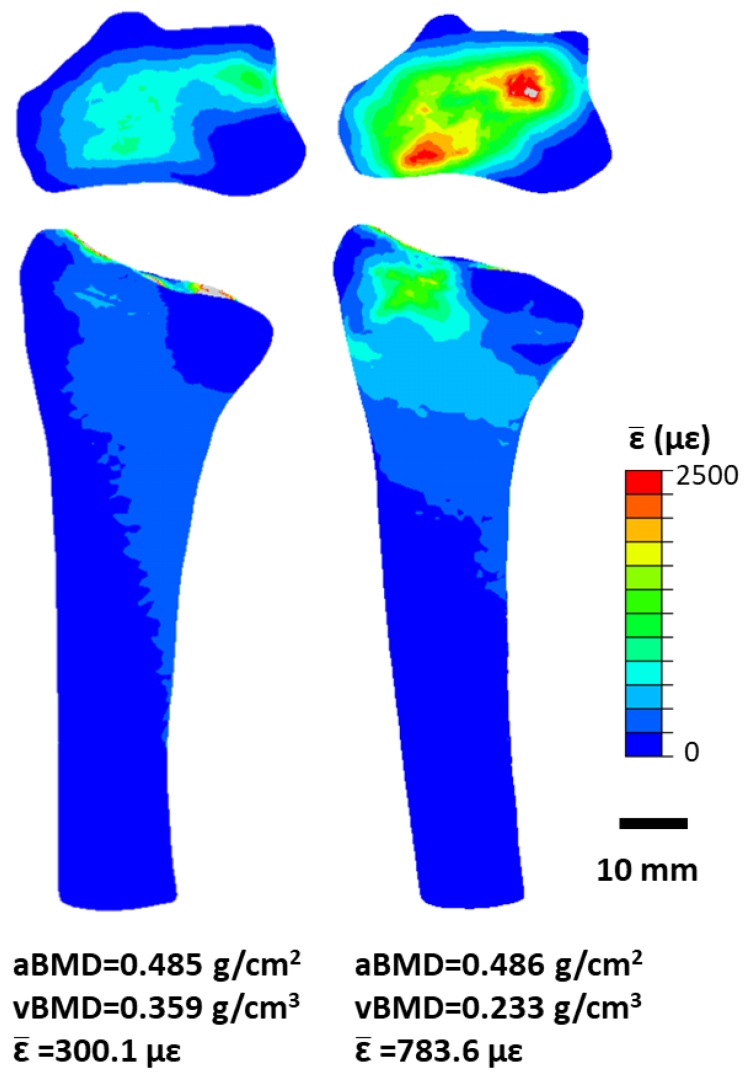
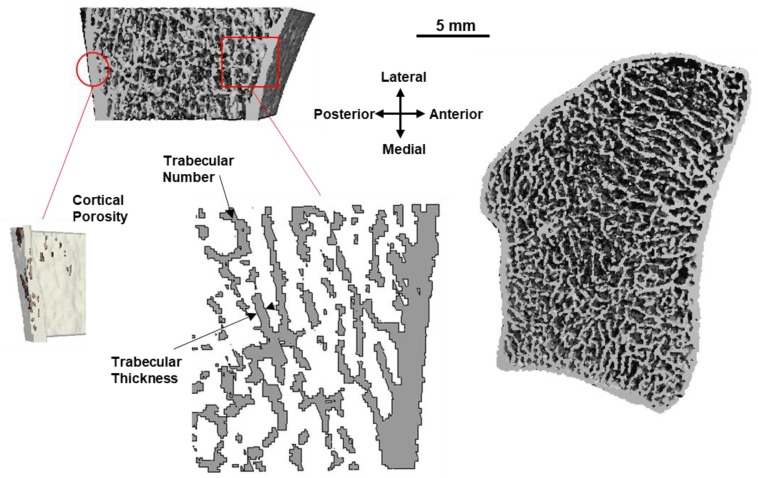
Keywords: areal bone mineral density; bone adaptation; bone mineral density; high resolution peripheral quantitative computed tomography; mechanical loading; quantitative computed tomography; structure; volumetric bone mineral density.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- United States Bone and Joint Initiative . In: The Burden of Musculoskeletal Diseases in the United States. 3rd ed. Saag K., Wright N.C., Kilgore M., editors. American Academy or Orthopaedic Surgeons; Rosemont, IL, USA: 2014.
-
- National Osteoporosis Foundation Osteoporosis Exercise for Strong Bones. [(accessed on 3 March 2018)]; Available online: https://www.nof.org/patients/fracturesfall-prevention/exercisesafe-movem...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
