

Association of Pulse Wave Velocity With Chronic Kidney Disease Progression and Mortality: Findings From the CRIC Study (Chronic Renal Insufficiency Cohort)
- PMID: 29712736
- PMCID: PMC6342478
- DOI: 10.1161/HYPERTENSIONAHA.117.10648
Association of Pulse Wave Velocity With Chronic Kidney Disease Progression and Mortality: Findings From the CRIC Study (Chronic Renal Insufficiency Cohort)
Abstract
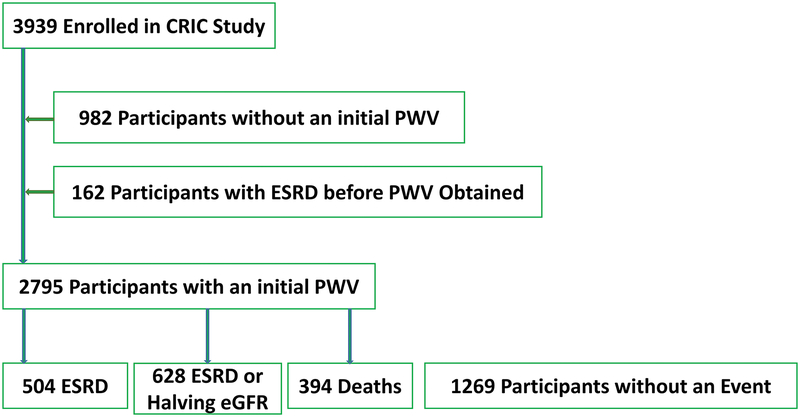
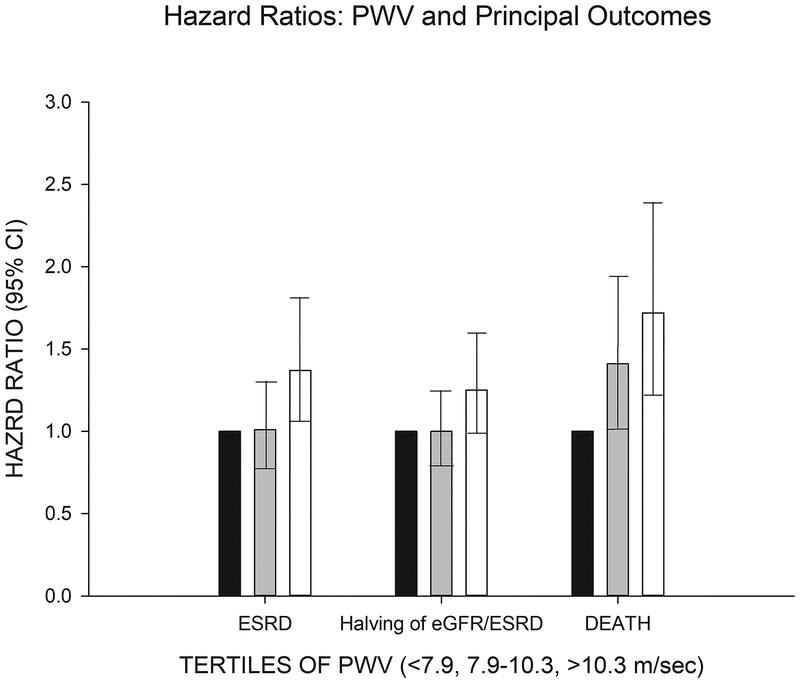
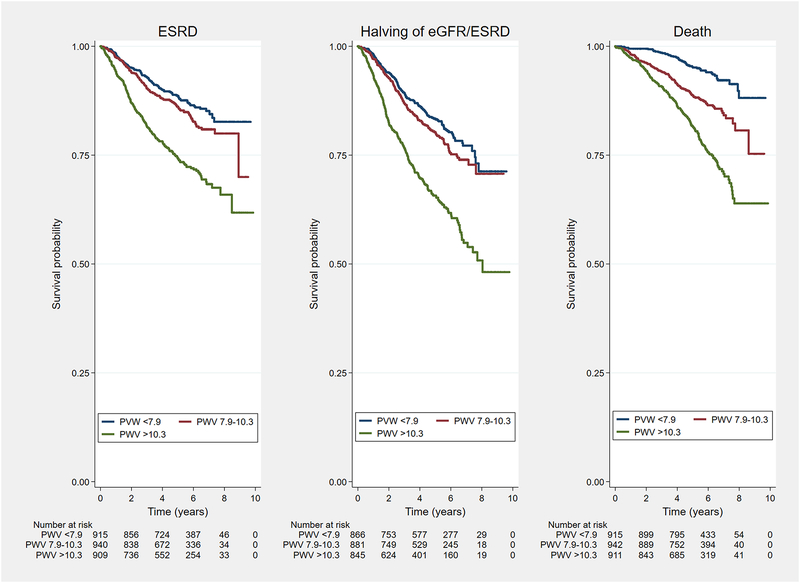
Patients with chronic kidney diseases (CKDs) are at risk for further loss of kidney function and death, which occur despite reasonable blood pressure treatment. To determine whether arterial stiffness influences CKD progression and death, independent of blood pressure, we conducted a prospective cohort study of CKD patients enrolled in the CRIC study (Chronic Renal Insufficiency Cohort). Using carotid-femoral pulse wave velocity (PWV), we examined the relationship between PWV and end-stage kidney disease (ESRD), ESRD or halving of estimated glomerular filtration rate, or death from any cause. The 2795 participants we enrolled had a mean age of 60 years, 56.4% were men, 47.3% had diabetes mellitus, and the average estimated glomerular filtration rate at entry was 44.4 mL/min per 1.73 m2 During follow-up, there were 504 ESRD events, 628 ESRD or halving of estimated glomerular filtration rate events, and 394 deaths. Patients with the highest tertile of PWV (>10.3 m/s) were at higher risk for ESRD (hazard ratio [95% confidence interval], 1.37 [1.05-1.80]), ESRD or 50% decline in estimated glomerular filtration rate (hazard ratio [95% confidence interval], 1.25 [0.98-1.58]), or death (hazard ratio [95% confidence interval], 1.72 [1.24-2.38]). PWV is a significant predictor of CKD progression and death in people with impaired kidney function. Incorporation of PWV measurements may help define better the risks for these important health outcomes in patients with CKDs. Interventions that reduce aortic stiffness deserve study in people with CKD.
Keywords: follow-up studies; humans; kidney failure, chronic; renal insufficiency, chronic; vascular stiffness.
© 2018 American Heart Association, Inc.
Conflict of interest statement
Disclosures and Conflicts of Interest
Raymond R. Townsend, MD: NIH grants, Consultant to Medtronic and Janssen
Amanda Hyre Anderson, PhD
Julio A. Chirinos MD, PhD
Harold I. Feldman, MD NIH Grants, Kyowa Kirin (Speaker), Glaxo SmithKline (Speaker)
Juan Grunwald, MD
Lisa Nessel
Jason Roy, PhD
Boyang Chai, PhD
Matthew Weir, MD NIH Grants, Janssen, Astra Zeneca, MSD, Akebia, Boston Scientific, Relypsa, Boeheinger-Ingelheim, Bayer
Mahboob Rahman, MD
Jackson T Wright, Jr, MD NIH Grants
Nisha Bansal, MD
Chi-yuan Hsu, MD, MSc
John Kusek, PhD
Figures
References
-
- Hashimoto J, Ito S. Central pulse pressure and aortic stiffness determine renal hemodynamics: pathophysiological implication for microalbuminuria in hypertension. Hypertension 2011; 58:839–846. - PubMed
-
- O’Rourke MF, Safar ME. Relationship between aortic stiffening and microvascular disease in brain and kidney: cause and logic of therapy. Hypertension 2005; 46:200–204. - PubMed
-
- Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Ford CE, Shulman NB, Stamler J. Blood pressure and end-stage renal disease in men. Clinical Nephrology 1996; 334:13–18. - PubMed
-
- Anderson AH, Yang W, Townsend RR, Pan Q, Chertow GM, Kusek JW, Charleston J, He J, Kallem R, Lash JP, Miller ER III, Rahman M, Steigerwalt S, Weir M, Wright JT Jr., Feldman HI. Time-updated systolic blood pressure and the progression of chronic kidney disease: a cohort study. Ann Intern Med 2015; 162:258–265. - PMC - PubMed
-
- Guerin AP, Blacher J, Pannier B, Marchais SJ, Safar ME, London GM. Impact of aortic stiffness attenuation on survival of patients in end-stage renal failure. Circulation 2001; 103:987–992. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK061028/DK/NIDDK NIH HHS/United States
- R01 DK072231/DK/NIDDK NIH HHS/United States
- R01 DK067390/DK/NIDDK NIH HHS/United States
- K01 DK092353/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- G20 RR030969/RR/NCRR NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- KL2 RR024130/RR/NCRR NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- C06 RR028609/RR/NCRR NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- UL1 TR002003/TR/NCATS NIH HHS/United States
- KL2 RR029878/RR/NCRR NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1 RR024986/RR/NCRR NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- KL2 RR024987/RR/NCRR NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
