

Elevated urinary N-acetyl-β-D-glucosaminidase is associated with high glycoalbumin-to-hemoglobin A1c ratio in type 1 diabetes patients with early diabetic kidney disease
- PMID: 29712934
- PMCID: PMC5928247
- DOI: 10.1038/s41598-018-25023-5
Elevated urinary N-acetyl-β-D-glucosaminidase is associated with high glycoalbumin-to-hemoglobin A1c ratio in type 1 diabetes patients with early diabetic kidney disease
Abstract
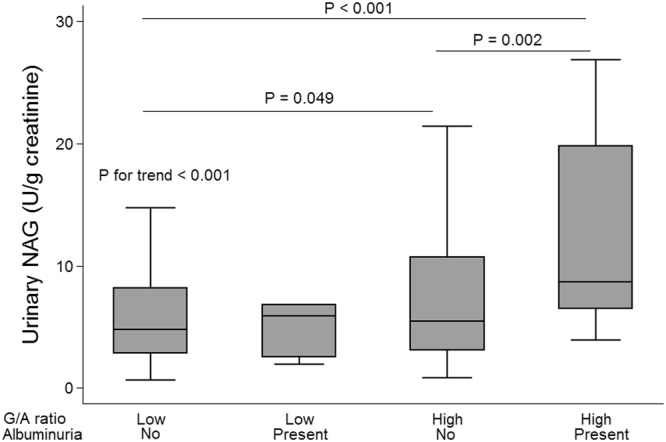
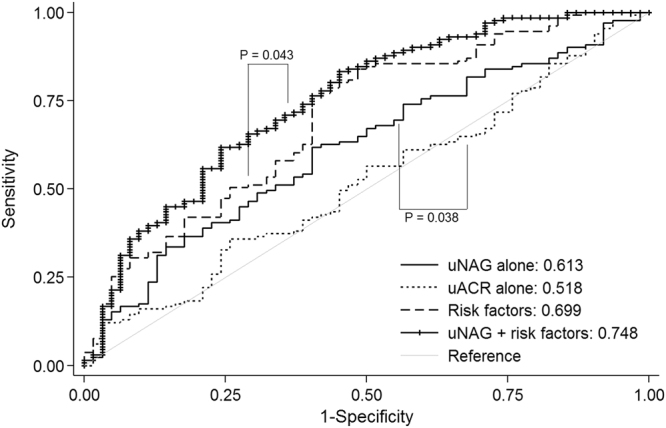
Urinary N-acetyl-β-D-glucosaminidase (uNAG) predicted the progression of diabetic kidney disease (DKD) prior to development of albuminuria in diabetes patients. We sought whether uNAG level is associated with glycoalbumin-to-hemoglobin A1c ratio (G/A ratio), a marker of postprandial hyperglycemia and glycemic excursion, independent of albuminuria and kidney function. The association between uNAG excretion and G/A ratio was assessed in 204 consecutive subjects with type 1 diabetes (T1D) (mean age 43.9 years; 49.0% men). uNAG excretion level increased along with older age, hyperglycemia, and degree of albuminuria, but was not correlated with body mass index or estimated glomerular filtration rate (eGFR). Elevated uNAG showed robust association with higher G/A ratio (adjusted β = 0.103, P = 0.020) after adjustment for age, sex, body mass index, duration of diabetes, uACR, angiotensin blockers use, fasting plasma glucose, and hemoglobin level. uNAG showed better discriminatory performance for individuals with high G/A ratio than albuminuria (AUC 0.613 vs. 0.518, P = 0.038). Measurement of uNAG improved AUC for high G/A ratio from 0.699 to 0.748 (P = 0.043) when added to conventional risk factors (cutoff 5.24 U/g creatinine; sensitivity 62.5% and specificity 58.0%). In conclusion, Elevated uNAG was found to be associated with high G/A ratio in patients with T1D with early stage DKD, independent of age and albuminuria.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Elevated N-acetyl-β-d-glucosaminidase, a urinary tubular damage marker, is a significant predictor of carotid artery atherosclerosis in type 1 diabetes, independent of albuminuria: A cross-sectional study.J Diabetes Complications. 2018 Aug;32(8):777-783. doi: 10.1016/j.jdiacomp.2018.05.019. Epub 2018 Jun 1. J Diabetes Complications. 2018. PMID: 29980431
-
Association between nonalbumin proteinuria and renal tubular damage of N-acetyl-β-d-glucosaminidase and its clinical relevance in patients with type 2 diabetes without albuminuria.J Diabetes Complications. 2019 Mar;33(3):255-260. doi: 10.1016/j.jdiacomp.2018.09.010. Epub 2018 Sep 15. J Diabetes Complications. 2019. PMID: 30236543
-
Urinary N-acetyl-β-D-glucosaminidase, an early marker of diabetic kidney disease, might reflect glucose excursion in patients with type 2 diabetes.Medicine (Baltimore). 2016 Jul;95(27):e4114. doi: 10.1097/MD.0000000000004114. Medicine (Baltimore). 2016. PMID: 27399115 Free PMC article.
-
Clinical impact of glycated albumin as another glycemic control marker.Endocr J. 2010;57(9):751-62. doi: 10.1507/endocrj.k10e-138. Epub 2010 Aug 17. Endocr J. 2010. PMID: 20724796 Review.
-
Diabetic Kidney Disease: Is There a Role for Glycemic Variability?Curr Diab Rep. 2018 Feb 15;18(3):13. doi: 10.1007/s11892-018-0979-3. Curr Diab Rep. 2018. PMID: 29450720 Review.
Cited by
-
Significance of Diabetic Kidney Disease Biomarkers in Predicting Metabolic-Associated Fatty Liver Disease.Biomedicines. 2023 Jul 7;11(7):1928. doi: 10.3390/biomedicines11071928. Biomedicines. 2023. PMID: 37509567 Free PMC article. Review.
-
Codonopsis tangshen Oliv. Amelioration Effect on Diabetic Kidney Disease Rats Induced by High Fat Diet Feeding Combined with Streptozotocin.Nat Prod Bioprospect. 2018 Dec;8(6):441-451. doi: 10.1007/s13659-018-0187-5. Epub 2018 Nov 1. Nat Prod Bioprospect. 2018. PMID: 30387083 Free PMC article.
-
Nephroprotective Effects of Tetramethylpyrazine Nitrone TBN in Diabetic Kidney Disease.Front Pharmacol. 2021 Jun 24;12:680336. doi: 10.3389/fphar.2021.680336. eCollection 2021. Front Pharmacol. 2021. PMID: 34248629 Free PMC article.
-
GA/HbA1c ratio is a simple and practical indicator to evaluate the risk of metabolic dysfunction-associated fatty liver disease in type 2 diabetes: an observational study.Diabetol Metab Syndr. 2022 Nov 11;14(1):167. doi: 10.1186/s13098-022-00946-2. Diabetol Metab Syndr. 2022. PMID: 36369095 Free PMC article.
-
L-shaped association between the GA/HbA1c ratio and all-cause mortality in U.S. adults with NAFLD: a cross-sectional study from the NHANES 1999-2004.BMC Endocr Disord. 2024 Mar 11;24(1):35. doi: 10.1186/s12902-024-01568-7. BMC Endocr Disord. 2024. PMID: 38468235 Free PMC article.
References
-
- Stevens PE, Levin A. & Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group, M. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013;158:825–830. doi: 10.7326/0003-4819-158-11-201306040-00007. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
