

Magnetic Resonance Venography Findings of Obstructed Hepatic Veins and the Inferior Vena Cava in Patients with Budd-Chiari Syndrome
- PMID: 29713215
- PMCID: PMC5904464
- DOI: 10.3348/kjr.2018.19.3.381
Magnetic Resonance Venography Findings of Obstructed Hepatic Veins and the Inferior Vena Cava in Patients with Budd-Chiari Syndrome
Abstract
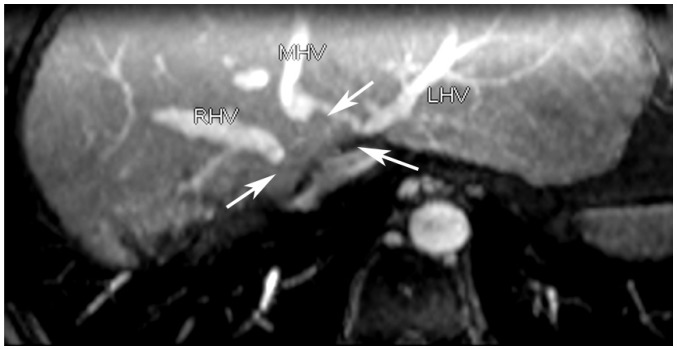
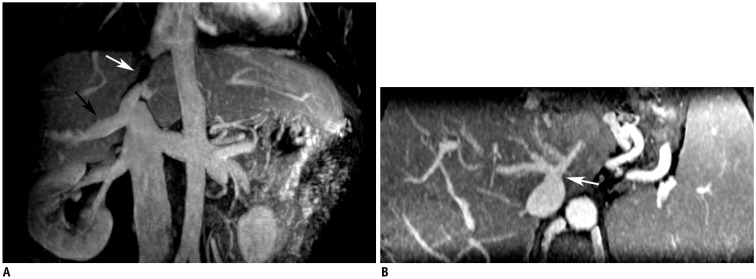
Objective: This study aimed to illustrate the magnetic resonance venography (MRV) manifestations of obstructed hepatic veins (HVs), the inferior vena cava (IVC), and accessory hepatic veins (AHVs) in patients with Budd-Chiari syndrome (BCS) and to evaluate the visualization capacity of MRV in the diagnosis of BCS.
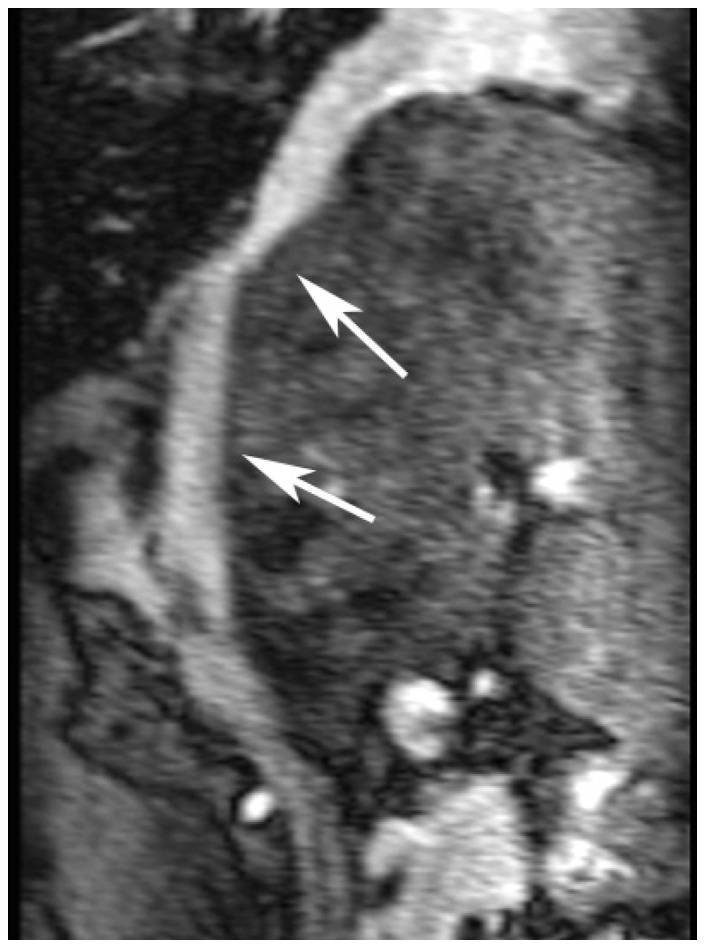
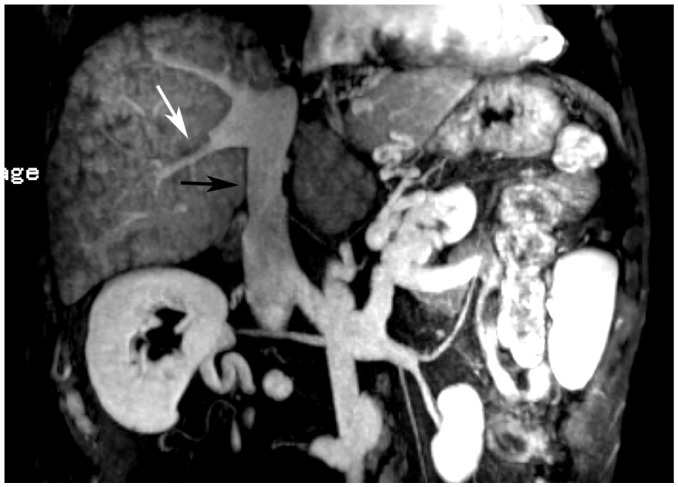
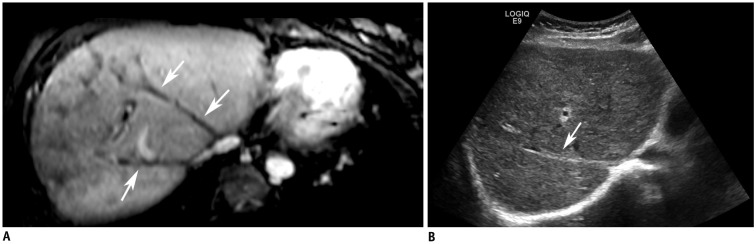
Materials and methods: Fifty-two patients with chronic BCS were included in this study. All patients were examined via MRV performed with a 3T system following injections of gadolinium-diethylene triamine pentaacetic acid (Gd-DTPA) or Gd-ethoxibenzyl-DTPA. HV and IVC lesions were classified, and their characteristics were described. HV cord-like occlusions detected via MRV were compared using ultrasonography (US). Digital subtraction angiography (DSA) was performed as a contrast in the MRV detection of IVC lesions. The HVs draining collaterals, mainly AHVs, were carefully observed. HV lesions were classified as segmental stenosis, segmental occlusion, membranous stenosis, membranous occlusion, cord-like occlusion, or non-visualized. Except for patent IVCs, IVC lesions were classified as segmental occlusion, segmental stenosis, membranous occlusion, membranous stenosis, and hepatomegaly-induced stenosis.
Results: All patients (52/52, 100%) showed HV lesions of different degrees. MRV was inferior to US in detecting cord-like occlusions (6 vs. 19, χ2 = 11.077, p < 0.001). Dilated AHVs, including 50 (50/52, 96.2%) caudate lobe veins and 37 (37/52, 71.2%) inferior HV and AHV lesions, were well-detected. There were no significant differences in detecting segmental lesions and thrombosis between MRV and DSA (χ2 = 0.000, p1 = 1.000, p2 = 1.000). The capacity of MRV to detect membranous lesions was inferior to that of DSA (7 vs. 15, χ2 = 6.125, p = 0.013).
Conclusion: In patients with BCS, MRV can clearly display the lesions in HVs and the IVC, as well as in AHVs, and it has diagnostic and therapeutic value.
Keywords: Angiography; Budd-Chiari syndrome; Hepatic vein; Inferior vena cava; MOVC; Magnetic resonance imaging; Venography.
Figures


Similar articles
-
Ultrasonographic Visualization of Accessory Hepatic Veins and Their Lesions in Budd-Chiari Syndrome.Ultrasound Med Biol. 2015 Aug;41(8):2091-8. doi: 10.1016/j.ultrasmedbio.2015.03.023. Epub 2015 May 4. Ultrasound Med Biol. 2015. PMID: 25952161
-
[Budd-Chiari syndrome in children and adolescents: therapeutic radiological intervention].Zhonghua Er Ke Za Zhi. 2013 Aug;51(8):590-4. Zhonghua Er Ke Za Zhi. 2013. PMID: 24225289 Chinese.
-
Non-contrast-enhanced MR angiography in the diagnosis of Budd-Chiari syndrome (BCS) compared with digital subtraction angiography (DSA): Preliminary results.Magn Reson Imaging. 2017 Feb;36:7-11. doi: 10.1016/j.mri.2016.10.006. Epub 2016 Oct 11. Magn Reson Imaging. 2017. PMID: 27742430
-
Sonography in Budd-Chiari syndrome.J Ultrasound Med. 2006 Mar;25(3):373-9. doi: 10.7863/jum.2006.25.3.373. J Ultrasound Med. 2006. PMID: 16495498 Review.
-
Budd-Chiari syndrome: imaging review.Br J Radiol. 2018 Dec;91(1092):20180441. doi: 10.1259/bjr.20180441. Epub 2018 Jul 24. Br J Radiol. 2018. PMID: 30004805 Free PMC article. Review.
Cited by
-
Diagnostic accuracy of Doppler ultrasound, CT and MRI in Budd Chiari syndrome: systematic review and meta-analysis.Br J Radiol. 2020 May 1;93(1109):20190847. doi: 10.1259/bjr.20190847. Epub 2020 Mar 18. Br J Radiol. 2020. PMID: 32150462 Free PMC article.
References
-
- Hefaiedh R, Cheikh M, Marsaoui L, Ennaifer R, Romdhane H, Ben Nejma H, et al. The Budd-Chiari syndrome. Tunis Med. 2013;91:376–281. - PubMed
-
- Hidaka M, Eguchi S. Budd-Chiari syndrome: focus on surgical treatment. Hepatol Res. 2017;47:142–148. - PubMed
-
- Klein AS. Management of Budd-Chiari syndrome. Liver Transpl. 2006;12:S23–S28. - PubMed
-
- Valla DC. Primary Budd-Chiari syndrome. J Hepatol. 2009;50:195–203. - PubMed
-
- Gai YH. [Sonographic classification of blood-drainage in Budd-Chiari syndrome with hepatic vein obstruction] Chin J UItrasonogr. 2008;6:517–520.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
