

Pelvic MRI: Is Endovaginal or Rectal Filling Needed?
- PMID: 29713217
- PMCID: PMC5904466
- DOI: 10.3348/kjr.2018.19.3.397
Pelvic MRI: Is Endovaginal or Rectal Filling Needed?
Abstract
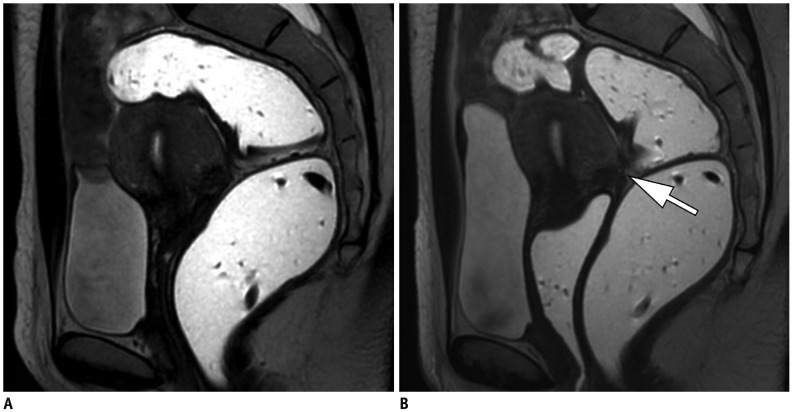
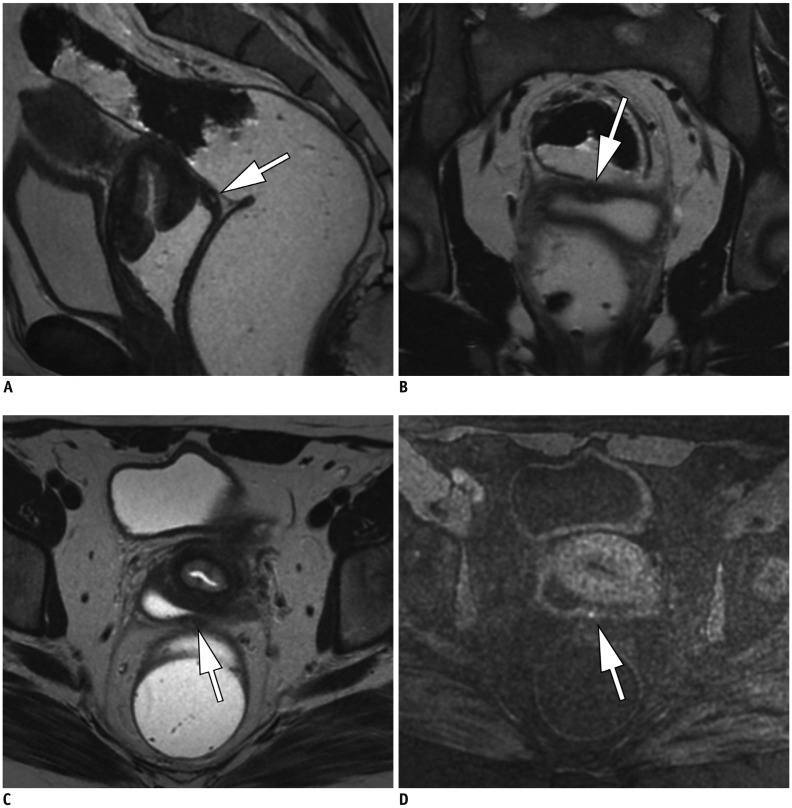
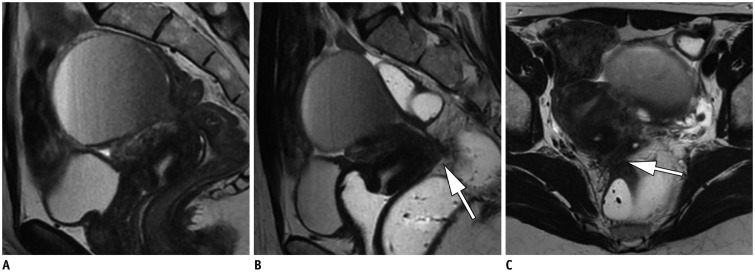
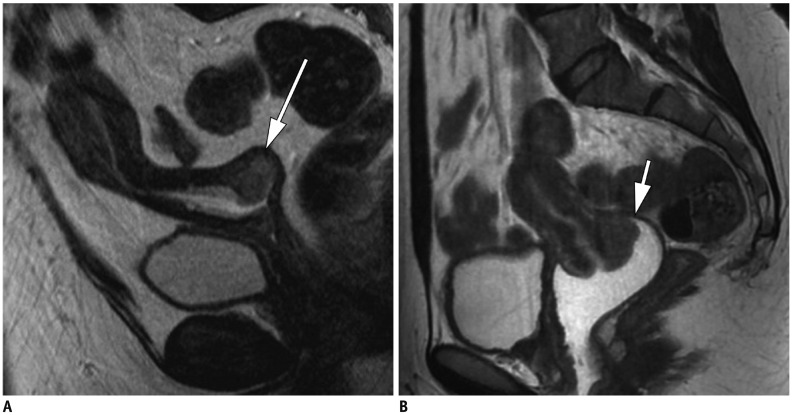
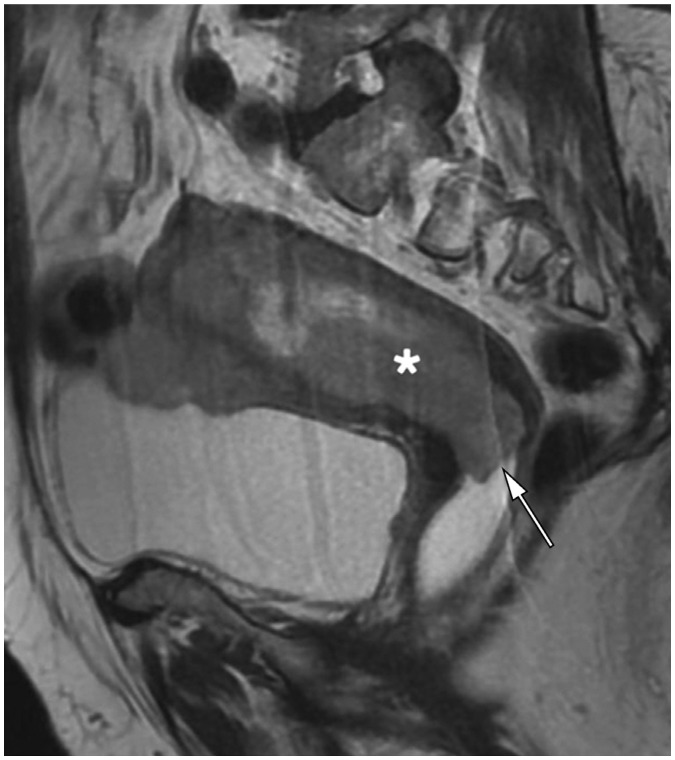
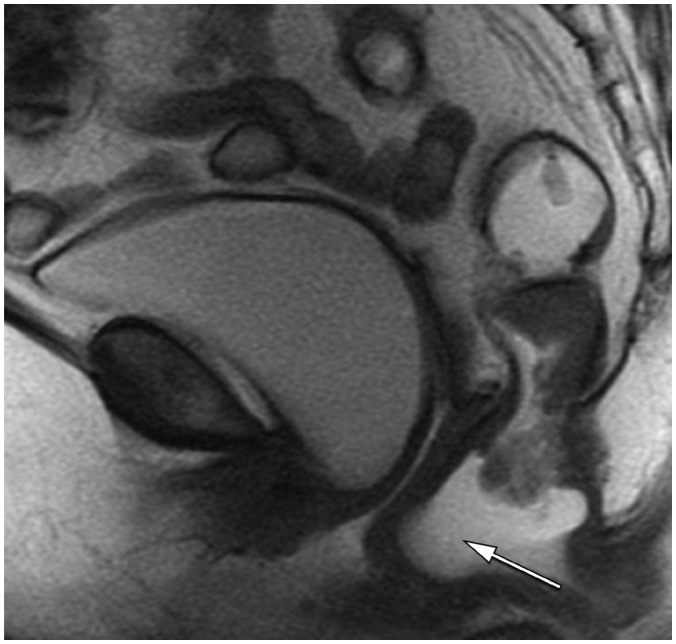
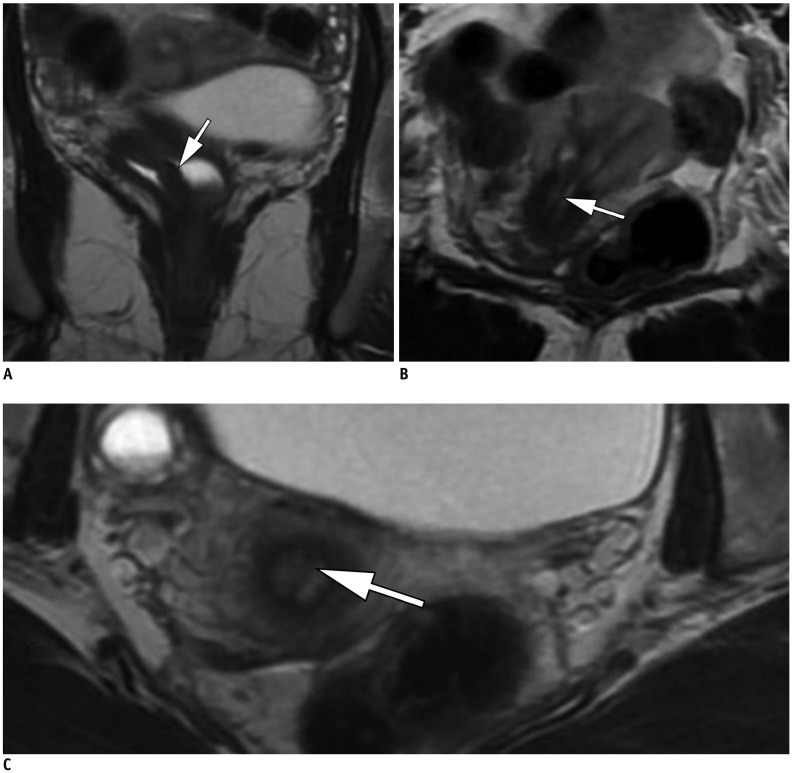
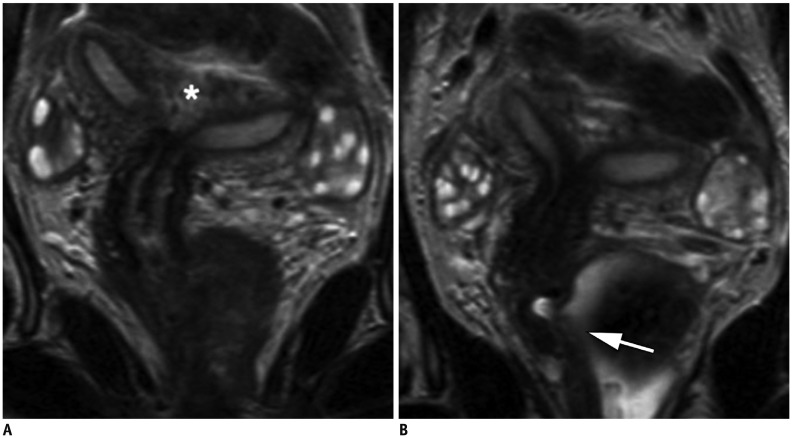
Magnetic resonance imaging is the optimal modality for pelvic imaging. It is based on T2-weighted magnetic resonance (MR) sequences allowing uterine and vaginal cavity assessment as well as rectal evaluation. Anatomical depiction of these structures may benefit from distension, and conditions either developing inside the lumen of cavities or coming from the outside may then be better delineated and localized. The need for distension, either rectal or vaginal, and the way to conduct it are matters of debate, depending on indication for which the MR examination is being conducted. In this review, we discuss advantages and potential drawbacks of this technique, based on literature and our experience, in the evaluation of various gynecological and rectal diseases.
Keywords: Endoluminal contrast; GI imaging; GU imaging; Magnetic resonace imaging; Pelvic organ prolapse.
Figures



References
-
- Lienemann A, Fischer T. Functional imaging of the pelvic floor. Eur J Radiol. 2003;47:117–122. - PubMed
-
- Bitti GT, Argiolas GM, Ballicu N, Caddeo E, Cecconi M, Demurtas G, et al. Pelvic floor failure: MR imaging evaluation of anatomic and functional abnormalities. Radiographics. 2014;34:429–448. - PubMed
-
- Marchiolè P, Cittadini G, Sala P, Moioli M, Mathevet P, Capaccio E, et al. Pre- and post-operative work-up in patients affected by early cervical cancer and eligible for fertilitysparing treatment: role of MRI with saline hydrocolpos. Abdom Imaging. 2010;35:271–279. - PubMed
-
- Maccioni F. Functional disorders of the ano-rectal compartment of the pelvic floor: clinical and diagnostic value of dynamic MRI. Abdom Imaging. 2013;38:930–951. - PubMed
-
- Hetzer FH, Andreisek G, Tsagari C, Sahrbacher U, Weishaupt D. MR defecography in patients with fecal incontinence: imaging findings and their effect on surgical management. Radiology. 2006;240:449–457. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
