

Altered White Matter Integrity in Human Immunodeficiency Virus-Associated Neurocognitive Disorder: A Tract-Based Spatial Statistics Study
- PMID: 29713221
- PMCID: PMC5904470
- DOI: 10.3348/kjr.2018.19.3.431
Altered White Matter Integrity in Human Immunodeficiency Virus-Associated Neurocognitive Disorder: A Tract-Based Spatial Statistics Study
Abstract
Objective: Human immunodeficiency virus (HIV) infection has been known to damage the microstructural integrity of white matter (WM). However, only a few studies have assessed the brain regions in HIV-associated neurocognitive disorders (HAND) with diffusion tensor imaging (DTI). Therefore, we sought to compare the DTI data between HIV patients with and without HAND using tract-based spatial statistics (TBSS).
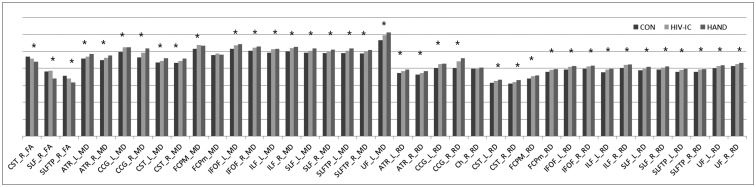
Materials and methods: Twenty-two HIV-infected patients (10 with HAND and 12 without HAND) and 11 healthy controls (HC) were enrolled in this study. A whole-brain analysis of fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity was performed with TBSS and a subsequent 20 tract-specific region-of-interest (ROI)-based analysis to localize and compare altered WM integrity in all group contrasts.
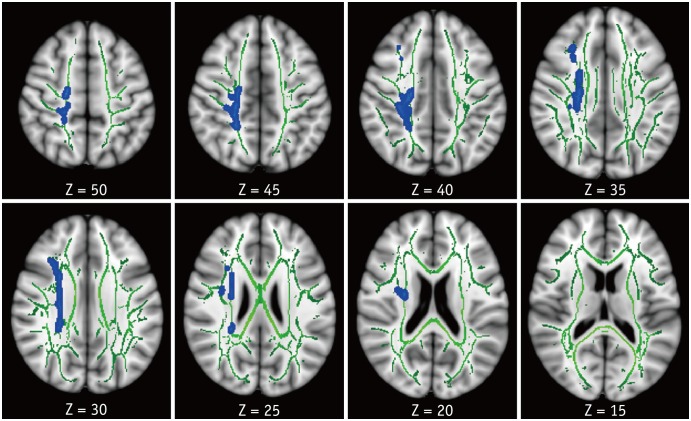
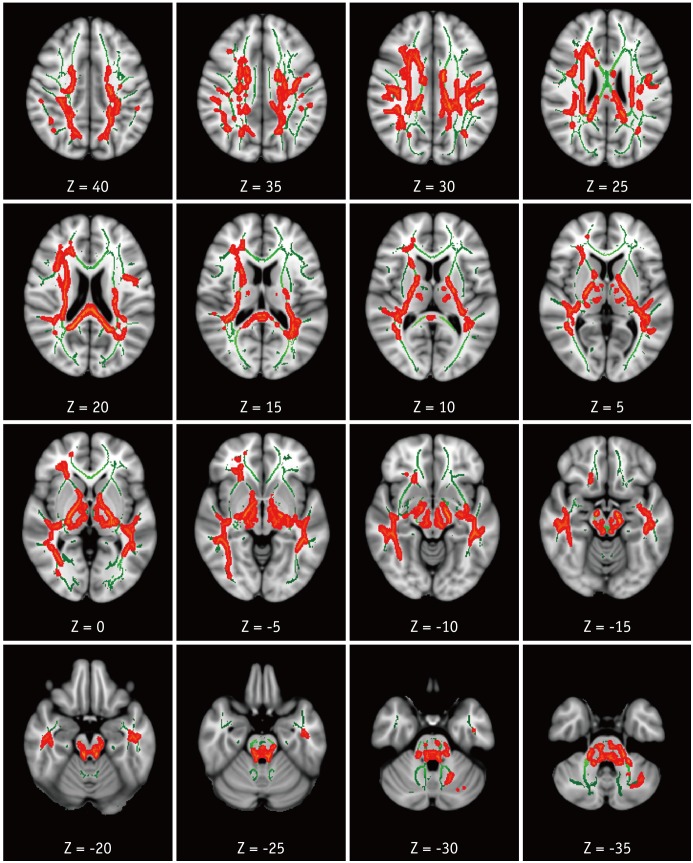
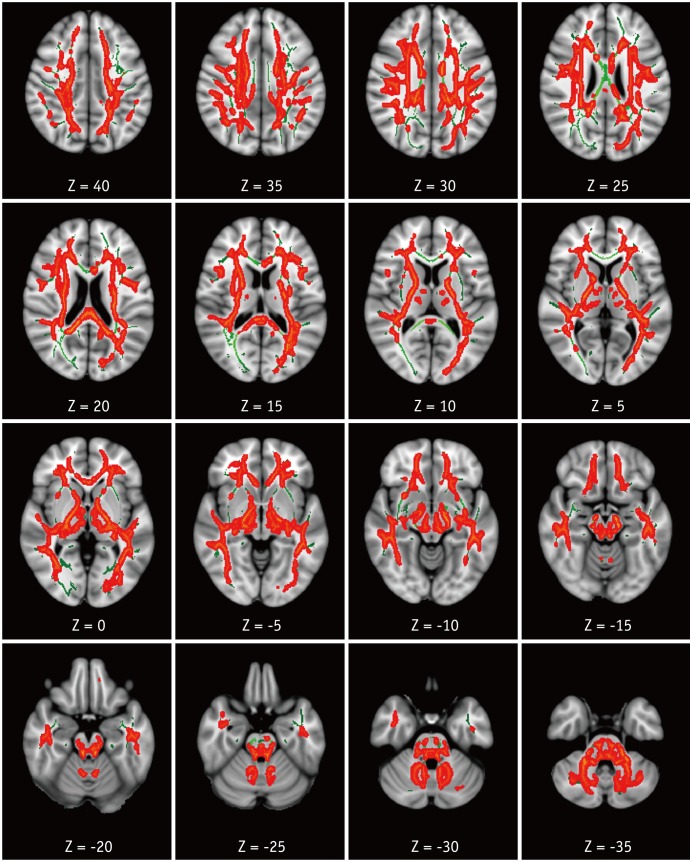
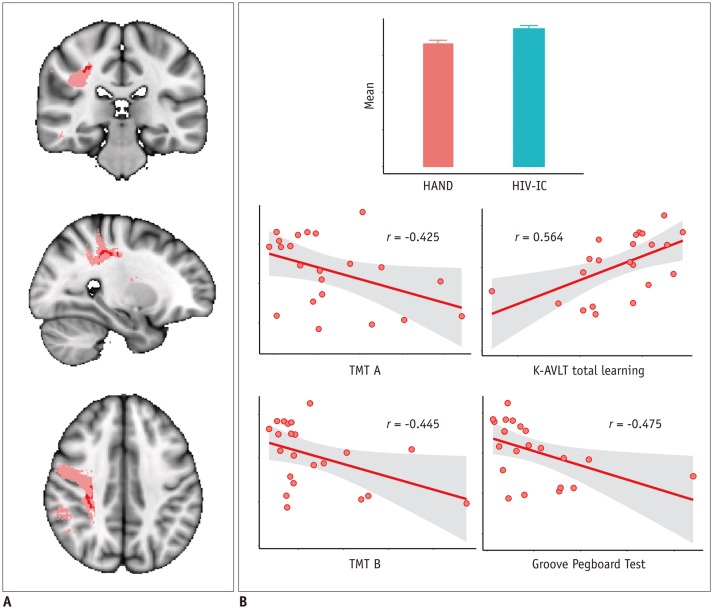
Results: Compared with HC, patients with HAND showed decreased FA in the right frontoparietal WM including the upper corticospinal tract (CST) and increased MD and RD in the bilateral frontoparietal WM, corpus callosum, bilateral CSTs and bilateral cerebellar peduncles. The DTI values did not significantly differ between HIV patients with and without HAND or between HIV patients without HAND and HC. In the ROI-based analysis, decreased FA was observed in the right superior longitudinal fasciculus and was significantly correlated with decreased information processing speed, memory, executive function, and fine motor function in HIV patients.
Conclusion: These results suggest that altered integrity of the frontoparietal WM contributes to cognitive dysfunction in HIV patients.
Keywords: Diffusion tensor imaging; HIV; HIV-associated neurocognitive disorders (HAND); Human immunodeficiency virus; TBSS.
Figures
Similar articles
-
Altered white matter integrity in patients with monocular blindness: A diffusion tensor imaging and tract-based spatial statistics study.Brain Behav. 2020 Aug;10(8):e01720. doi: 10.1002/brb3.1720. Epub 2020 Jun 17. Brain Behav. 2020. PMID: 32558355 Free PMC article.
-
Microstructural white matter abnormalities in hypothyroidism evaluation with diffusion tensor imaging tract-based spatial statistical analysis.Radiol Med. 2021 Feb;126(2):283-290. doi: 10.1007/s11547-020-01234-7. Epub 2020 Jun 10. Radiol Med. 2021. PMID: 32524282
-
The role of diffusion tensor imaging and fractional anisotropy in the evaluation of patients with idiopathic normal pressure hydrocephalus: a literature review.Neurosurg Focus. 2016 Sep;41(3):E12. doi: 10.3171/2016.6.FOCUS16192. Neurosurg Focus. 2016. PMID: 27581308 Review.
-
Gray and white matter alterations in early HIV-infected patients: Combined voxel-based morphometry and tract-based spatial statistics.J Magn Reson Imaging. 2016 Jun;43(6):1474-83. doi: 10.1002/jmri.25100. Epub 2015 Dec 30. J Magn Reson Imaging. 2016. PMID: 26714822
-
White matter microstructural damage in early treated phenylketonuric patients.Orphanet J Rare Dis. 2018 Oct 26;13(1):188. doi: 10.1186/s13023-018-0912-5. Orphanet J Rare Dis. 2018. PMID: 30367646 Free PMC article.
Cited by
-
Minocycline attenuation of rat corpus callosum abnormality mediated by low-dose lipopolysaccharide-induced microglia activation.J Neuroinflammation. 2021 Apr 26;18(1):100. doi: 10.1186/s12974-021-02142-x. J Neuroinflammation. 2021. PMID: 33902641 Free PMC article.
-
Neuroimaging advances in neurocognitive disorders among HIV-infected individuals.Front Neurol. 2025 Feb 13;16:1479183. doi: 10.3389/fneur.2025.1479183. eCollection 2025. Front Neurol. 2025. PMID: 40017532 Free PMC article. Review.
-
Exosomal MicroRNAs Associate With Neuropsychological Performance in Individuals With HIV Infection on Antiretroviral Therapy.J Acquir Immune Defic Syndr. 2019 Dec 15;82(5):514-522. doi: 10.1097/QAI.0000000000002187. J Acquir Immune Defic Syndr. 2019. PMID: 31714431 Free PMC article.
-
Biomarkers of Activation and Inflammation to Track Disparity in Chronological and Physiological Age of People Living With HIV on Combination Antiretroviral Therapy.Front Immunol. 2020 Oct 9;11:583934. doi: 10.3389/fimmu.2020.583934. eCollection 2020. Front Immunol. 2020. PMID: 33162998 Free PMC article. Review.
-
Altered white matter microstructure and neurocognitive function of HIV-infected patients with low nadir CD4.J Neurovirol. 2022 Jun;28(3):355-366. doi: 10.1007/s13365-022-01053-8. Epub 2022 Jul 1. J Neurovirol. 2022. PMID: 35776340
References
-
- Schouten J, Cinque P, Gisslen M, Reiss P, Portegies P. HIV-1 infection and cognitive impairment in the cART era: a review. AIDS. 2011;25:561–575. - PubMed
-
- Dore GJ, McDonald A, Li Y, Kaldor JM, Brew BJ National HIV Surveillance Committee. Marked improvement in survival following AIDS dementia complex in the era of highly active antiretroviral therapy. AIDS. 2003;17:1539–1545. - PubMed
-
- Chernoff RA, Martin DJ, Schrock DA, Huy MP. Neuropsychological functioning as a predictor of employment activity in a longitudinal study of HIV-infected adults contemplating workforce reentry. J Int Neuropsychol Soc. 2010;16:38–48. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
