

Diameter of the Solid Component in Subsolid Nodules on Low-Dose Unenhanced Chest Computed Tomography: Measurement Accuracy for the Prediction of Invasive Component in Lung Adenocarcinoma
- PMID: 29713229
- PMCID: PMC5904478
- DOI: 10.3348/kjr.2018.19.3.508
Diameter of the Solid Component in Subsolid Nodules on Low-Dose Unenhanced Chest Computed Tomography: Measurement Accuracy for the Prediction of Invasive Component in Lung Adenocarcinoma
Abstract
Objective: To determine if measurement of the diameter of the solid component in subsolid nodules (SSNs) on low-dose unenhanced chest computed tomography (CT) is as accurate as on standard-dose enhanced CT in prediction of pathological size of invasive component of lung adenocarcinoma.
Materials and methods: From February 2012 to October 2015, 114 SSNs were identified in 105 patients that underwent low-dose unenhanced and standard-dose enhanced CT pre-operatively. Three radiologists independently measured the largest diameter of the solid component. Intraclass correlation coefficients (ICCs) were used to assess inter-reader agreement. We estimated measurement differences between the size of solid component and that of invasive component. We measured diagnostic accuracy of the prediction of invasive adenocarcinoma using a size criterion of a solid component ≥ 6 mm, and compared them using a generalized linear mixed model.
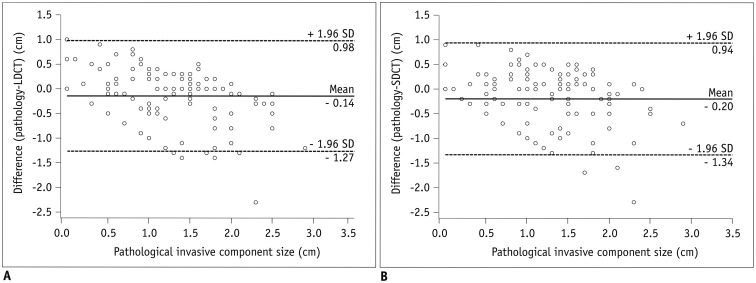
Results: Inter-reader agreement was excellent (ICC, 0.84.0.89). The mean ± standard deviation of absolute measurement differences between the solid component and invasive component was 4 ± 4 mm in low-dose unenhanced CT and 5 ± 4 mm in standard-dose enhanced CT. Diagnostic accuracy was 81.3% (95% confidence interval, 76.7.85.3%) in low-dose unenhanced CT and 76.6% (71.8.81.0%) in standard-dose enhanced CT, with no statistically significant difference (p = 0.130).
Conclusion: Measurement of the diameter of the solid component of SSNs on low-dose unenhanced chest CT was as accurate as on standard-dose enhanced CT for predicting the invasive component. Thus, low-dose unenhanced CT may be used safely in the evaluation of patients with SSNs.
Keywords: Invasive component; Low-dose CT; Lung adenocarcinoma; Measurement; Subsolid nodule.
Figures
Similar articles
-
Nodule Classification on Low-Dose Unenhanced CT and Standard-Dose Enhanced CT: Inter-Protocol Agreement and Analysis of Interchangeability.Korean J Radiol. 2018 May-Jun;19(3):516-525. doi: 10.3348/kjr.2018.19.3.516. Epub 2018 Apr 6. Korean J Radiol. 2018. PMID: 29713230 Free PMC article.
-
Effect of computed tomography window settings and reconstruction plane on 8th edition T-stage classification in patients with lung adenocarcinoma manifesting as a subsolid nodule.Eur J Radiol. 2018 Jan;98:130-135. doi: 10.1016/j.ejrad.2017.11.015. Epub 2017 Nov 22. Eur J Radiol. 2018. PMID: 29279151
-
Improving the prediction of lung adenocarcinoma invasive component on CT: Value of a vessel removal algorithm during software segmentation of subsolid nodules.Eur J Radiol. 2018 Mar;100:58-65. doi: 10.1016/j.ejrad.2018.01.016. Epub 2018 Jan 31. Eur J Radiol. 2018. PMID: 29496080
-
Subsolid pulmonary nodules: imaging evaluation and strategic management.Curr Opin Pulm Med. 2012 Jul;18(4):304-12. doi: 10.1097/MCP.0b013e328354a5f2. Curr Opin Pulm Med. 2012. PMID: 22575798 Review.
-
Overview and strategic management of subsolid pulmonary nodules.J Thorac Imaging. 2012 Jul;27(4):240-8. doi: 10.1097/RTI.0b013e31825d515b. J Thorac Imaging. 2012. PMID: 22847591 Review.
Cited by
-
A radiomics nomogram for invasiveness prediction in lung adenocarcinoma manifesting as part-solid nodules with solid components smaller than 6 mm.Front Oncol. 2022 Aug 11;12:900049. doi: 10.3389/fonc.2022.900049. eCollection 2022. Front Oncol. 2022. PMID: 36033463 Free PMC article.
-
Comparative genomics between matched solid and lepidic portions of semi-solid lung adenocarcinomas.Lung Cancer. 2023 Jun;180:107211. doi: 10.1016/j.lungcan.2023.107211. Epub 2023 Apr 21. Lung Cancer. 2023. PMID: 37121213 Free PMC article.
-
Characteristics of Recent Articles Published in the Korean Journal of Radiology Based on the Citation Frequency.Korean J Radiol. 2020 Dec;21(12):1284. doi: 10.3348/kjr.2020.1322. Korean J Radiol. 2020. PMID: 33236548 Free PMC article. No abstract available.
-
Gross handling of pulmonary resection specimen: maintaining the 3-dimensional orientation.J Thorac Dis. 2019 Jan;11(Suppl 1):S37-S44. doi: 10.21037/jtd.2018.12.36. J Thorac Dis. 2019. PMID: 30775026 Free PMC article. Review.
-
Comparative validation of clinical staging based on solid component versus total tumor size in resected lung adenocarcinoma.Eur Radiol. 2025 May 24. doi: 10.1007/s00330-025-11668-0. Online ahead of print. Eur Radiol. 2025. PMID: 40411551
References
-
- Goo JM, Park CM, Lee HJ. Ground-glass nodules on chest CT as imaging biomarkers in the management of lung adenocarcinoma. AJR Am J Roentgenol. 2011;196:533–543. - PubMed
-
- Rami-Porta R, Bolejack V, Crowley J, Ball D, Kim J, Lyons G, et al. The IASLC lung cancer staging project: proposals for the revisions of the T descriptors in the forthcoming eighth edition of the TNM classification for lung cancer. J Thorac Oncol. 2015;10:990–1003. - PubMed
-
- Travis WD, Asamura H, Bankier AA, Beasley MB, Detterbeck F, Flieder DB, et al. The IASLC lung cancer staging project: proposals for coding T categories for subsolid nodules and assessment of tumor size in part-solid tumors in the forthcoming eighth edition of the TNM classification of lung cancer. J Thorac Oncol. 2016;11:1204–1223. - PubMed
-
- Lee HY, Choi YL, Lee KS, Han J, Zo JI, Shim YM, et al. Pure ground-glass opacity neoplastic lung nodules: histopathology, imaging, and management. AJR Am J Roentgenol. 2014;202:W224–W233. - PubMed
-
- Hwang EJ, Park CM, Ryu Y, Lee SM, Kim YT, Kim YW, et al. Pulmonary adenocarcinomas appearing as part-solid ground-glass nodules: is measuring solid component size a better prognostic indicator? Eur Radiol. 2015;25:558–567. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
