

Comparative Prospective Study Reporting Intraoperative Parameters, Pedicle Screw Perforation, and Radiation Exposure in Navigation-Guided versus Non-navigated Fluoroscopy-Assisted Minimal Invasive Transforaminal Lumbar Interbody Fusion
- PMID: 29713413
- PMCID: PMC5913023
- DOI: 10.4184/asj.2018.12.2.309
Comparative Prospective Study Reporting Intraoperative Parameters, Pedicle Screw Perforation, and Radiation Exposure in Navigation-Guided versus Non-navigated Fluoroscopy-Assisted Minimal Invasive Transforaminal Lumbar Interbody Fusion
Abstract
Study design: Prospective cohort study.
Purpose: To compare intraoperative parameters, radiation exposure, and pedicle screw perforation rate in navigation-guided versus non-navigated fluoroscopy-assisted minimal invasive transforaminal lumbar interbody fusion (MIS TLIF).
Overview of literature: The poor reliability of fluoroscopy-guided instrumentation and growing concerns about radiation exposure have led to the development of navigation-guided instrumentation techniques in MIS TLIF. The literature evaluating the efficacy of navigation-guided MIS TLIF is scant.
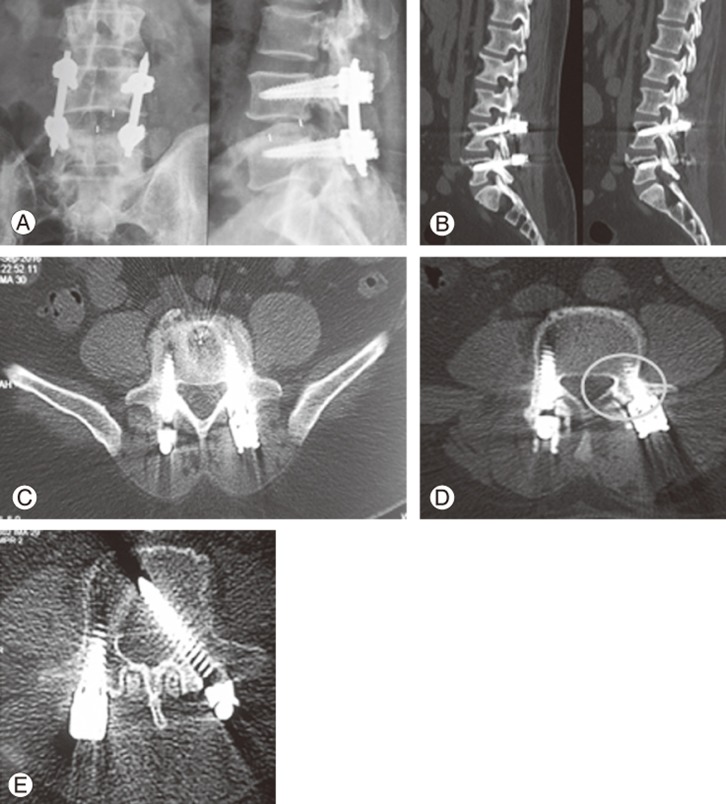
Methods: Eighty-seven patients underwent navigation- or fluoroscopy-guided MIS TLIF for symptomatic lumbar/lumbosacral spondylolisthesis. Demographics, intraoperative parameters (surgical time, blood loss), and radiation exposure (sec/mGy/Gy.cm2 noted from C-arm for comparison only) were recorded. Computed tomography was performed in patients in the navigation and non-navigation groups at postoperative 12 months and reviewed by an independent observer to assess the accuracy of screw placement, perforation incidence, location, grade (Mirza), and critical versus non-critical neurological implications.
Results: Twenty-seven patients (male/female, 11/16; L4-L5/L5-S1, 9/18) were operated with navigation-guided MIS TLIF, whereas 60 (male/female, 25/35; L4-L5/L5-S1, 26/34) with conventional fluoroscopy-guided MIS TILF. The use of navigation resulted in reduced fluoroscopy usage (dose area product, 0.47 Gy.cm2 versus 2.93 Gy.cm2), radiation exposure (1.68 mGy versus 10.97 mGy), and fluoroscopy time (46.5 seconds versus 119.08 seconds), with p-values of <0.001. Furthermore, 96.29% (104/108) of pedicle screws in the navigation group were accurately placed (grade 0) (4 breaches, all grade I) compared with 91.67% (220/240) in the non-navigation group (20 breaches, 16 grade I+4 grade II; p=0.114). None of the breaches resulted in a corresponding neurological deficit or required revision.
Conclusions: Navigation guidance in MIS TLIF reduced radiation exposure, but the perforation status was not statistically different than that for the fluoroscopy-based technique. Thus, navigation in nondeformity cases is useful for significantly reducing the radiation exposure, but its ability to reduce pedicle screw perforation in nondeformity cases remains to be proven.
Keywords: Computer-assisted; Fusion; Minimal invasive surgical procedures; Radiation exposure; Spondylolisthesis.
Conflict of interest statement
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Ravi B, Zahrai A, Rampersaud R. Clinical accuracy of computer-assisted two-dimensional fluoroscopy for the percutaneous placement of lumbosacral pedicle screws. Spine (Phila Pa 1976) 2011;36:84–91. - PubMed
-
- Kosmopoulos V, Schizas C. Pedicle screw placement accuracy: a meta-analysis. Spine (Phila Pa 1976) 2007;32:E111–E120. - PubMed
-
- Esses SI, Sachs BL, Dreyzin V. Complications associated with the technique of pedicle screw fixation: a selected survey of ABS members. Spine (Phila Pa 1976) 1993;18:2231–2238. - PubMed
-
- Lonstein JE, Denis F, Perra JH, Pinto MR, Smith MD, Winter RB. Complications associated with pedicle screws. J Bone Joint Surg Am. 1999;81:1519–1528. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
