

Zinc as an adjunct therapy in the management of severe pneumonia among Gambian children: randomized controlled trial
- PMID: 29713463
- PMCID: PMC5908397
- DOI: 10.7189/jogh.08.010418
Zinc as an adjunct therapy in the management of severe pneumonia among Gambian children: randomized controlled trial
Abstract
Background: The benefit of zinc as an adjunct therapy for severe pneumonia is not established. We assessed the benefit of adjunct zinc therapy for severe pneumonia in children and determined whether the study children were zinc deficient.
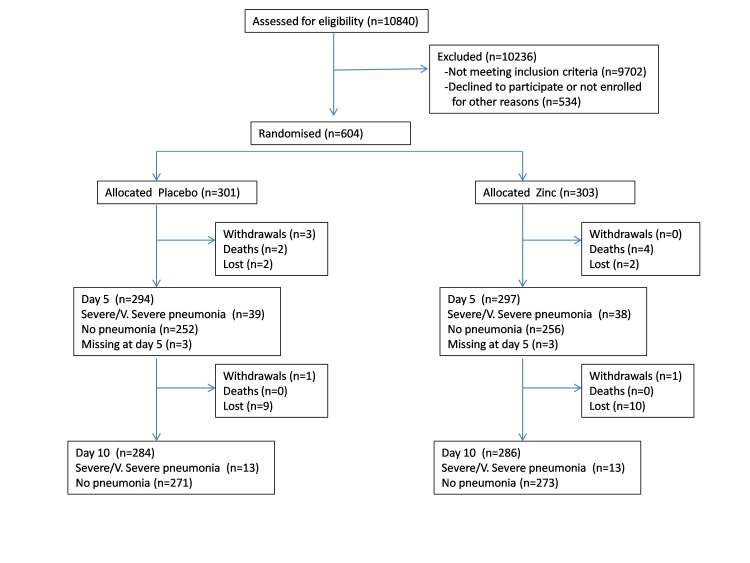
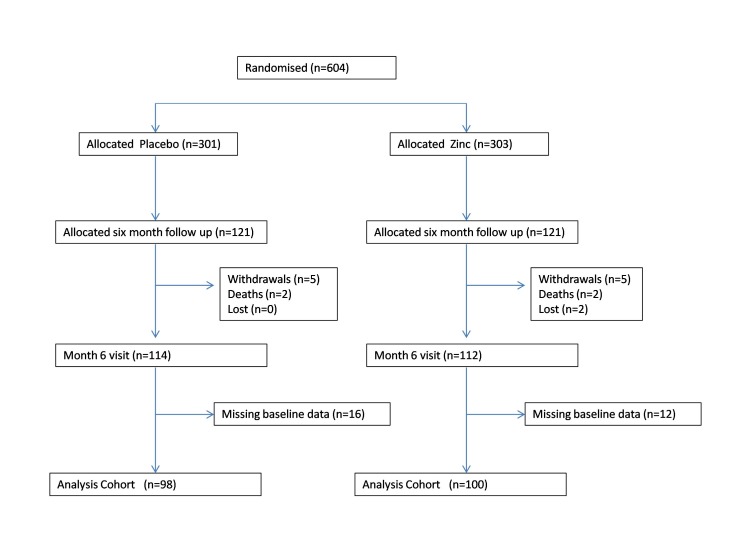
Methods: This was a randomized, parallel group, double-blind, placebo-controlled trial with an allocation ratio of 1:1 conducted in children with severe pneumonia to evaluate the efficacy of daily zinc as an adjunct treatment in preventing 'treatment failure' (presence of any sign of severe pneumonia) on day-5 and day-10 and in reducing the time to resolution of signs of severe pneumonia. Six hundred and four children 2-59 months of age presenting with severe pneumonia at six urban and rural health care facilities in The Gambia were individually randomised to receive placebo (n = 301) or zinc (n = 303) for seven days. To determine if the study children were zinc deficient, supplementation was continued in a randomly selected subgroup of 121 children from each arm for six months post-enrolment, and height-gain, nutritional status, plasma zinc concentrations, and immune competence were compared.
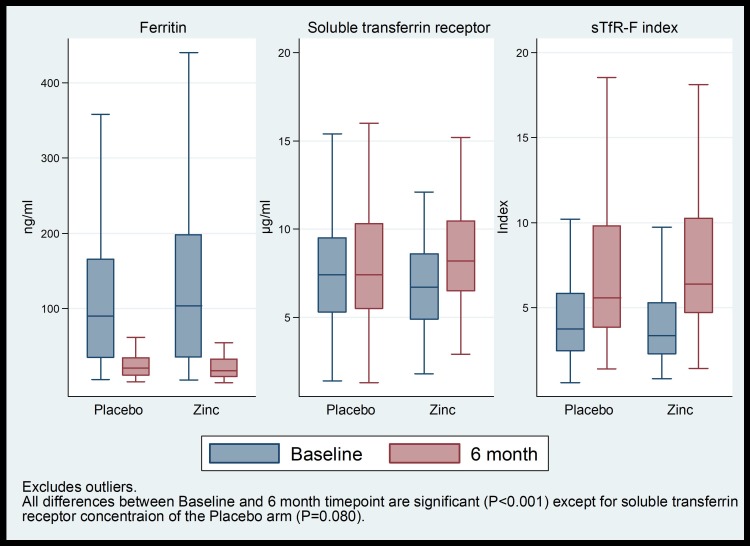
Results: Percentage of treatment failure were similar in placebo and zinc arms both on day 5 (14.0% vs 14.1%) and day 10 (5.2% vs 5.9%). The time to recovery from lower chest wall indrawing and sternal retraction was longer in the placebo compared to zinc arm (24.4 vs 23.0 hours; P = 0.011 and 18.7 vs 11.0 hours; P = 0.006 respectively). The time to resolution for all respiratory symptoms of severity was not significantly different between placebo and zinc arms (42.3 vs 30.9 hours respectively; P = 0.242). In the six months follow-up sub-group, there was no significant difference in height gain, height-for-age and weight-for-height Z-scores, mid upper arm circumference, plasma zinc concentrations, and anergy at six months post-enrolment.
Conclusions: In this population, zinc given as an adjunct treatment for severe pneumonia showed no benefit in treatment failure rates, or clinically important benefit in time to recovery from respiratory symptoms and showed marginal benefit in rapidity of resolution of some signs of severity. This finding does not support routine use of zinc as an adjunct treatment in severe pneumonia in generally zinc replete children.
Trial registration: ISRCTN33548493.
Conflict of interest statement
Competing interests: The authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflict of interest.
Figures
Similar articles
-
Zinc adjunct therapy reduces case fatality in severe childhood pneumonia: a randomized double blind placebo-controlled trial.BMC Med. 2012 Feb 8;10:14. doi: 10.1186/1741-7015-10-14. BMC Med. 2012. PMID: 22316073 Free PMC article. Clinical Trial.
-
Zinc as an adjunct to the treatment of severe pneumonia in Ecuadorian children: a randomized controlled trial.Am J Clin Nutr. 2014 Mar;99(3):497-505. doi: 10.3945/ajcn.113.067892. Epub 2014 Jan 15. Am J Clin Nutr. 2014. PMID: 24429536 Clinical Trial.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Role of zinc in severe pneumonia: a randomized double bind placebo controlled study.Ital J Pediatr. 2012 Aug 2;38:36. doi: 10.1186/1824-7288-38-36. Ital J Pediatr. 2012. PMID: 22856593 Free PMC article. Clinical Trial.
-
Efficacy of zinc given as an adjunct to the treatment of severe pneumonia: A meta-analysis of randomized, double-blind and placebo-controlled trials.Clin Respir J. 2018 Mar;12(3):857-864. doi: 10.1111/crj.12646. Epub 2017 May 31. Clin Respir J. 2018. PMID: 28488366 Review.
Cited by
-
Zinc against COVID-19? Symptom surveillance and deficiency risk groups.PLoS Negl Trop Dis. 2021 Jan 4;15(1):e0008895. doi: 10.1371/journal.pntd.0008895. eCollection 2021 Jan. PLoS Negl Trop Dis. 2021. PMID: 33395417 Free PMC article. Review.
-
Emergency care interventions for paediatric severe acute respiratory infections in low- and middle-income countries: A systematic review and narrative synthesis.J Glob Health. 2023 Jun 9;13:04065. doi: 10.7189/jogh.13.04065. J Glob Health. 2023. PMID: 37288550 Free PMC article.
-
Natural Ingredients to Improve Immunity.Pharmaceuticals (Basel). 2023 Apr 1;16(4):528. doi: 10.3390/ph16040528. Pharmaceuticals (Basel). 2023. PMID: 37111285 Free PMC article. Review.
-
Review of the role of additional treatments including oseltamivir, oral steroids, macrolides, and vitamin supplementation for children with severe pneumonia in low- and middle-income countries.J Glob Health. 2022 Aug 22;12:10005. doi: 10.7189/jogh.12.10005. J Glob Health. 2022. PMID: 35993199 Free PMC article. Review.
-
Zinc as an Adjuvant Therapy in Acute Severe Pneumonia in Children Aged Two Months to Two Years: A Double-Blind Randomized Controlled Trial.Cureus. 2025 Apr 16;17(4):e82402. doi: 10.7759/cureus.82402. eCollection 2025 Apr. Cureus. 2025. PMID: 40385774 Free PMC article.
References
-
- UN Inter-agency Group for Child Mortality Estimation. Levels & Trends in Child Mortality. 2015. Available: https://data.unicef.org/wp-content/uploads/2015/12/IGME-report-2015-chil.... Accessed: 29 November 2016.
-
- UN Inter-agency Group for Child Mortality Estimation. Cause of Death Data 2015. 2015. Available: https://data.unicef.org/topic/child-survival/under-five-mortality. Accessed: 29 November 2016.
-
- World Health Organization/The United Nations Children’s Fund (UNICEF). Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025 - The integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD). 2013. Available: http://www.unicef.org/media/files/Final_GAPPD_main_Report-_EN-8_April_20.... Accessed: 29 November 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
