

Postinfantile Giant Cell Hepatitis with Features of Acute Severe Autoimmune Hepatitis Probably Triggered by Diclofenac in a Patient with Primary Myelofibrosis
- PMID: 29713554
- PMCID: PMC5866856
- DOI: 10.1155/2018/9793868
Postinfantile Giant Cell Hepatitis with Features of Acute Severe Autoimmune Hepatitis Probably Triggered by Diclofenac in a Patient with Primary Myelofibrosis
Abstract
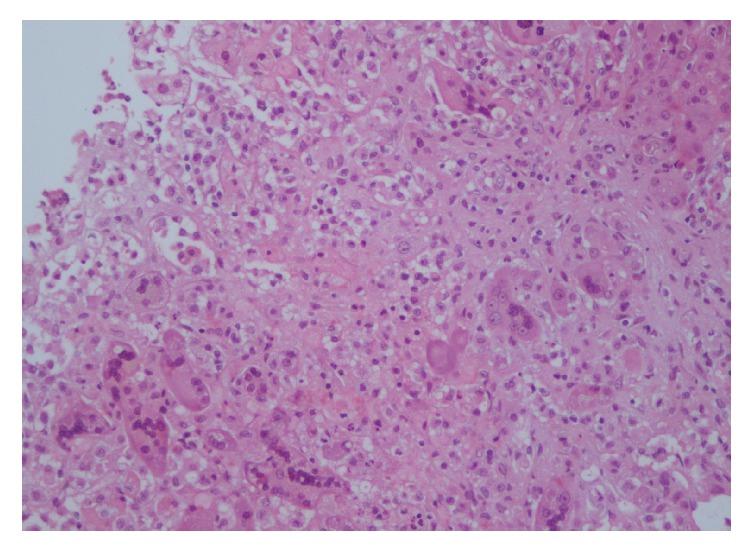
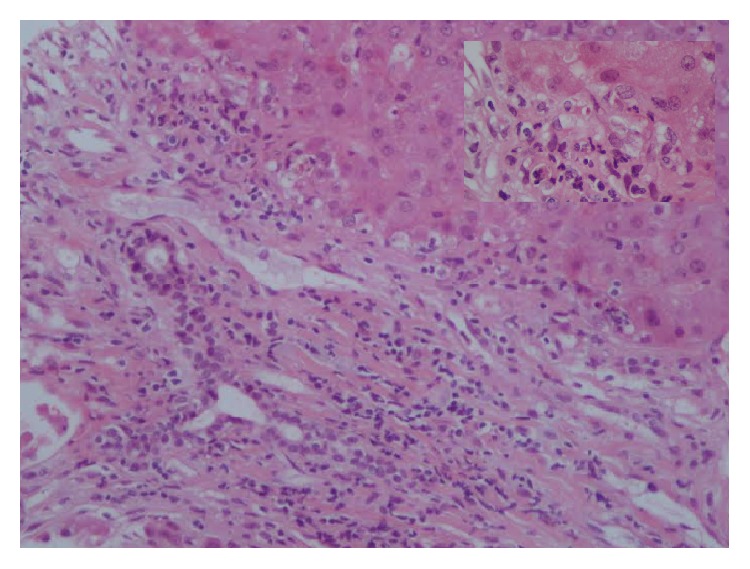
Giant cell hepatitis (GCH) is commonly reported in neonatal and infantile liver diseases but rarely in adults where the term postinfantile GCH (PIGCH) is used. PIGCH is associated with many diseases, including drugs toxicity, viruses, and autoimmune liver diseases, with autoimmune hepatitis (AIH) being the most prevalent. We present a case of PIGCH in a 76-year-old female without known history of liver disease who suffered from an acute severe episode of hepatitis. After careful exclusion of other hepatitis causes by imaging, virological, immunological, and microbiological investigations, a diagnosis of acute severe AIH (AS-AIH) was established. The patient was started on corticosteroids but she did not respond and died 3 days later because of advanced acute liver failure. Postmortem liver biopsy showed typical PIGCH lesions. Physicians must keep this catastrophic entity in mind in cases of unexplained acute liver injury as, contrary to our case, prompt rescue therapy with corticosteroids may be life-saving.
Figures
Similar articles
-
Postinfantile giant cell hepatitis in the setting of autoimmune hepatitis: exclusively a histological pattern or a prognosis predictor?BMJ Case Rep. 2021 Jul 21;14(7):e243660. doi: 10.1136/bcr-2021-243660. BMJ Case Rep. 2021. PMID: 34290027 Free PMC article.
-
Postinfantile Giant Cell Hepatitis in Native and Allograft Livers: A Multi-Institutional Clinicopathologic Study of 70 Cases.Mod Pathol. 2023 Nov;36(11):100298. doi: 10.1016/j.modpat.2023.100298. Epub 2023 Aug 6. Mod Pathol. 2023. PMID: 37544363
-
Postinfantile Giant Cell Hepatitis Secondary to Rheumatoid Arthritis.ACG Case Rep J. 2023 Apr 19;10(4):e01006. doi: 10.14309/crj.0000000000001006. eCollection 2023 Apr. ACG Case Rep J. 2023. PMID: 37091202 Free PMC article.
-
Autoimmune hepatitis with giant-cell transformation.Ann Hepatol. 2009 Jan-Mar;8(1):68-70. Ann Hepatol. 2009. PMID: 19221538 Review.
-
A fatal case of postinfantile giant cell hepatitis in a patient with chronic lymphocytic leukaemia.Eur J Gastroenterol Hepatol. 2003 May;15(5):551-5. doi: 10.1097/01.meg.0000050026.34359.7c. Eur J Gastroenterol Hepatol. 2003. PMID: 12702915 Review.
Cited by
-
Hellenic Association for the Study of the Liver Clinical Practice Guidelines: Autoimmune hepatitis.Ann Gastroenterol. 2019 Jan-Feb;32(1):1-23. doi: 10.20524/aog.2018.0330. Epub 2018 Nov 29. Ann Gastroenterol. 2019. PMID: 30598587 Free PMC article.
-
Postinfantile giant cell hepatitis in the setting of autoimmune hepatitis: exclusively a histological pattern or a prognosis predictor?BMJ Case Rep. 2021 Jul 21;14(7):e243660. doi: 10.1136/bcr-2021-243660. BMJ Case Rep. 2021. PMID: 34290027 Free PMC article.
-
Post-infantile Giant Cell Hepatitis: A Literature Review and Meta-analysis.J Clin Transl Pathol. 2022 Sep;2(3):100-107. doi: 10.14218/jctp.2022.00016. Epub 2022 Aug 31. J Clin Transl Pathol. 2022. PMID: 37092012 Free PMC article.
-
Asymptomatic giant cell hepatitis: a subtype of post-infantile giant cell hepatitis?Clin J Gastroenterol. 2019 Aug;12(4):367-371. doi: 10.1007/s12328-019-00950-6. Epub 2019 Feb 14. Clin J Gastroenterol. 2019. PMID: 30767175
-
Autoimmune post-infantile giant cell hepatitis: a case report and review of the literature.Can Liver J. 2021 Apr 29;4(2):104-109. doi: 10.3138/canlivj-2020-0024. eCollection 2021 Spring. Can Liver J. 2021. PMID: 35991767 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
