

Improving medication reconciliation at hospital admission, discharge and ambulatory care through a transition of care team
- PMID: 29713690
- PMCID: PMC5922563
- DOI: 10.1136/bmjoq-2017-000281
Improving medication reconciliation at hospital admission, discharge and ambulatory care through a transition of care team
Abstract
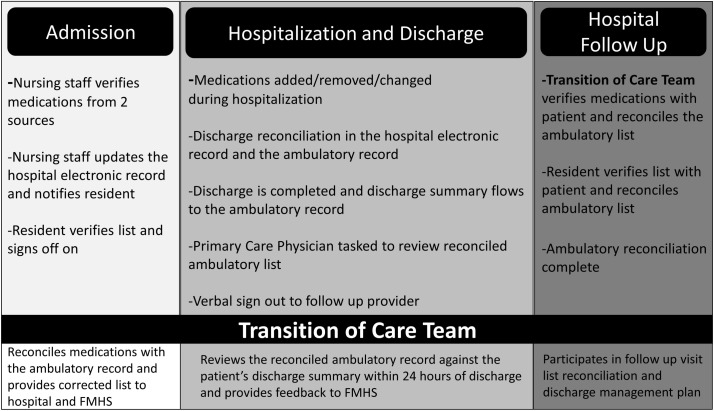
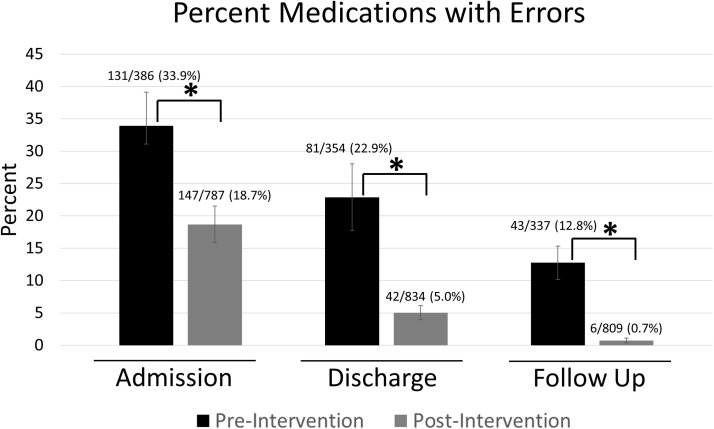
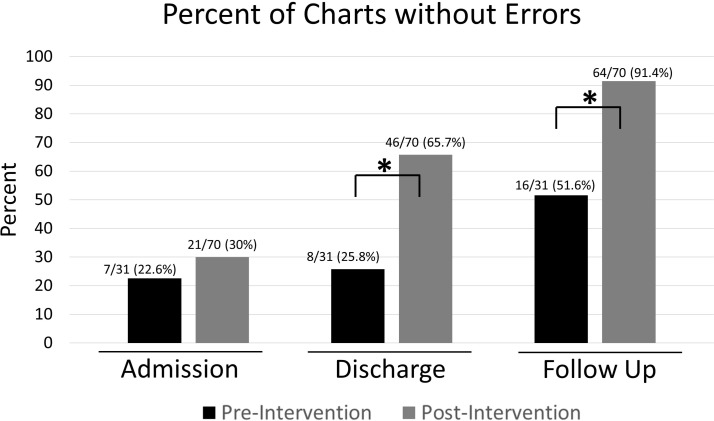
Medication reconciliation is an important component to the care of hospitalised patients and their safe transition to the ambulatory setting. In our Family Medicine Hospitalist Service, patient care is frequently transferred between the various physicians, residents, nurses and eventually to a separate group of providers who provide ambulatory management. Due to frequent transitions of care, there was no clear ownership of the medication reconciliation process. To improve the medication reconciliation process, a Transition of Care Team composed of registered nurses was created to oversee the entire reconciliation process. The team engaged the patient and their family, when needed, contacted patients' pharmacies and their providers, reconciled the patients' hospital medication list with the ambulatory list at hospital admission and within 24 hours of discharge, and attended the hospital follow-up visit to verify medications and provide continuity of care. Implementation of the team allowed for additional investigative resources, redundancy in preventing errors and early recovery should an error occur. The percent of medications with error after implementation of the Transition of Care Team was reduced from 131/386 (33.9%) to 147/787 (18.7%) at hospital admission, 81/354 (22.9%) to 42/834 (5.0%) at discharge and 43/337 (12.8%) to 6/809 (0.7%) at follow-up visit (two proportion tests, p<0.001). In addition, the percent of charts without any errors improved at hospital discharge from 8/31 (25.8%) to 46/70 (65.7%) and at hospital follow-up visit from 16/31 (51.6%) to 64/70 (91.4%) (two-proportion test, p<0.001). Previously viewed as three separate reconciliations occurring at admission, discharge and hospital follow-up, the approach to medication reconciliation was reframed as a continuous process occurring throughout the hospitalisation and hospital follow-up resulting in improved reconciliation accuracy and safer transitions to the ambulatory setting.
Keywords: ambulatory care; healthcare quality improvement; medication reconciliation; medication safety; six sigma.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Medication reconciliation in a rural trauma population.Ann Emerg Med. 2008 Nov;52(5):483-91. doi: 10.1016/j.annemergmed.2008.03.021. Epub 2008 Jun 12. Ann Emerg Med. 2008. PMID: 18550221
-
Medication reconciliation in continuum of care transitions: a moving target.J Am Med Dir Assoc. 2013 Sep;14(9):668-72. doi: 10.1016/j.jamda.2013.02.021. Epub 2013 Apr 19. J Am Med Dir Assoc. 2013. PMID: 23608529
-
[Medication reconciliation at admission and discharge. A consolidated experience].Rev Calid Asist. 2016 Jun;31 Suppl 1:45-54. doi: 10.1016/j.cali.2016.02.002. Epub 2016 May 4. Rev Calid Asist. 2016. PMID: 27157795 Spanish.
-
Preventing medication errors in transitions of care: A patient case approach.J Am Pharm Assoc (2003). 2015 Mar-Apr;55(2):e264-74; quiz e275-6. doi: 10.1331/JAPhA.2015.15509. J Am Pharm Assoc (2003). 2015. PMID: 25749270 Review.
-
Making inpatient medication reconciliation patient centered, clinically relevant and implementable: a consensus statement on key principles and necessary first steps.J Hosp Med. 2010 Oct;5(8):477-85. doi: 10.1002/jhm.849. J Hosp Med. 2010. PMID: 20945473
Cited by
-
Identification of kidney-related medications using AI from self-captured pill images.Ren Fail. 2024 Dec;46(2):2402075. doi: 10.1080/0886022X.2024.2402075. Epub 2024 Sep 11. Ren Fail. 2024. PMID: 39258385 Free PMC article.
-
Enhancing Transitions of Care: A Cross-Sectional Observational Study on the Role of Clinical Pharmacists in Transition Management in a Latin American Hospital.Cureus. 2024 Sep 9;16(9):e68998. doi: 10.7759/cureus.68998. eCollection 2024 Sep. Cureus. 2024. PMID: 39385894 Free PMC article.
-
Engineering care transitions: Clinician perceptions of barriers to safe medication management during transitions of patient care.Appl Ergon. 2021 Feb;91:103299. doi: 10.1016/j.apergo.2020.103299. Epub 2020 Nov 5. Appl Ergon. 2021. PMID: 33161183 Free PMC article.
-
Medication Discrepancies in Community Pharmacies in Switzerland: Identification, Classification, and Their Potential Clinical and Economic Impact.Pharmacy (Basel). 2020 Mar 9;8(1):36. doi: 10.3390/pharmacy8010036. Pharmacy (Basel). 2020. PMID: 32182863 Free PMC article.
-
A national survey on assessment of knowledge, perceptions, practice, and barriers among hospital pharmacists towards medication reconciliation in United Arab Emirates.Sci Rep. 2024 Jul 4;14(1):15370. doi: 10.1038/s41598-024-64605-4. Sci Rep. 2024. PMID: 38965258 Free PMC article.
References
-
- Makary MA, Daniel M. Medical error—the third leading cause of death in the US. BMJ 2016;353:i2139 doi:10.1136/bmj.i2139 - DOI - PubMed
-
- Roehr B. Institute of medicine report strives to reduce medication errors. BMJ 2006;333:220 doi:10.1136/bmj.333.7561.220-f - DOI - PMC - PubMed
-
- Kwan JL, Lo L, Sampson M, et al. . Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Ann Intern Med 2013;158:397–403. doi:10.7326/0003-4819-158-5-201303051-00006 - DOI - PubMed
-
- Rozich J, Resar R. Medication safety: one organization’s approach to the challenge. JCOM 2001;8:27–34.
-
- Aspden P, Wolcott J. Committee on Identifying and Preventing Medication Errors. Preventing medication errors: quality chasm series: The National Academies Press, 2007.
LinkOut - more resources
Full Text Sources
Other Literature Sources