

Coordination of Pharyngeal and Laryngeal Swallowing Events During Single Liquid Swallows After Oral Endotracheal Intubation for Patients with Acute Respiratory Distress Syndrome
- PMID: 29713897
- PMCID: PMC6207471
- DOI: 10.1007/s00455-018-9901-z
Coordination of Pharyngeal and Laryngeal Swallowing Events During Single Liquid Swallows After Oral Endotracheal Intubation for Patients with Acute Respiratory Distress Syndrome
Abstract
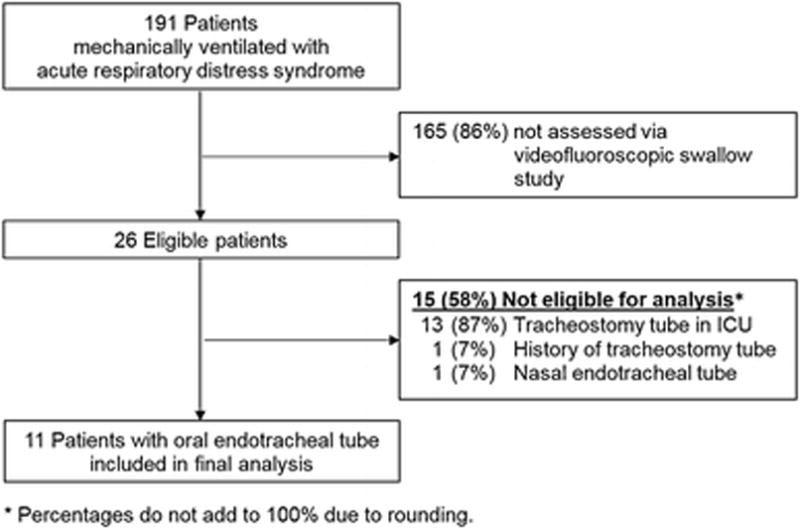
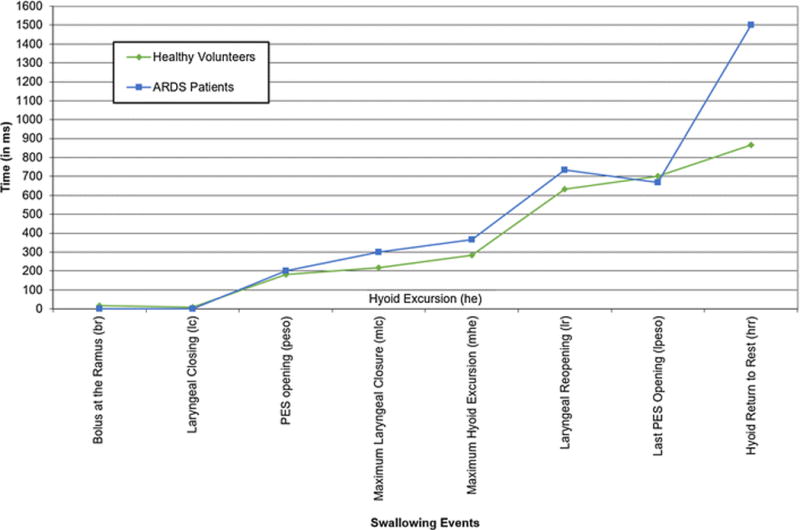
To evaluate timing and duration differences in airway protection and esophageal opening after oral intubation and mechanical ventilation for acute respiratory distress syndrome (ARDS) survivors versus age-matched healthy volunteers. Orally intubated adult (≥ 18 years old) patients receiving mechanical ventilation for ARDS were evaluated for swallowing impairments via a videofluoroscopic swallow study (VFSS) during usual care. Exclusion criteria were tracheostomy, neurological impairment, and head and neck cancer. Previously recruited healthy volunteers (n = 56) served as age-matched controls. All subjects were evaluated using 5-ml thin liquid barium boluses. VFSS recordings were reviewed frame-by-frame for the onsets of 9 pharyngeal and laryngeal events during swallowing. Eleven patients met inclusion criteria, with a median (interquartile range [IQR]) intubation duration of 14 (9, 16) days, and VFSSs completed a median of 5 (4, 13) days post-extubation. After arrival of the bolus in the pharynx, ARDS patients achieved maximum laryngeal closure a median (IQR) of 184 (158, 351) ms later than age-matched, healthy volunteers (p < 0.001) and it took longer to achieve laryngeal closure with a median (IQR) difference of 151 (103, 217) ms (p < 0.001), although there was no significant difference in duration of laryngeal closure. Pharyngoesophageal segment opening was a median (IQR) of - 116 (- 183, 1) ms (p = 0.004) shorter than in age-matched, healthy controls. Evaluation of swallowing physiology after oral endotracheal intubation in ARDS patients demonstrates slowed pharyngeal and laryngeal swallowing timing, suggesting swallow-related muscle weakness. These findings may highlight specific areas for further evaluation and potential therapeutic intervention to reduce post-extubation aspiration.
Keywords: Acute respiratory distress syndrome; Deglutition; Deglutition disorders; Dysphagia; Fluoroscopy; Intubation; Mechanical ventilation.
Conflict of interest statement
Conflict of Interest
All authors declare that there is no conflict of interest.
Figures
Similar articles
-
A Preliminary Videofluoroscopic Investigation of Swallowing Physiology and Function in Individuals with Oculopharyngeal Muscular Dystrophy (OPMD).Dysphagia. 2018 Dec;33(6):789-802. doi: 10.1007/s00455-018-9904-9. Epub 2018 May 3. Dysphagia. 2018. PMID: 29725764
-
Oral and pharyngeal bolus transit in patients with chronic obstructive pulmonary disease.Int J Chron Obstruct Pulmon Dis. 2015 Mar 5;10:489-96. doi: 10.2147/COPD.S74945. eCollection 2015. Int J Chron Obstruct Pulmon Dis. 2015. PMID: 25784795 Free PMC article.
-
Different types of dysphagia alleviated by the chin-down position.Auris Nasus Larynx. 2021 Oct;48(5):928-933. doi: 10.1016/j.anl.2021.02.008. Epub 2021 Feb 27. Auris Nasus Larynx. 2021. PMID: 33648799
-
Evaluation and treatment of swallowing disorders following endotracheal intubation and tracheostomy.Int Anesthesiol Clin. 2000 Summer;38(3):219-42. doi: 10.1097/00004311-200007000-00013. Int Anesthesiol Clin. 2000. PMID: 10984854 Review. No abstract available.
-
[Impairment of deglutition reflex after prolonged intubation].Ann Fr Anesth Reanim. 1992;11(1):17-21. doi: 10.1016/s0750-7658(05)80315-6. Ann Fr Anesth Reanim. 1992. PMID: 1443810 Review. French.
Cited by
-
The Association Between Endotracheal Tube Size and Aspiration (During Flexible Endoscopic Evaluation of Swallowing) in Acute Respiratory Failure Survivors.Crit Care Med. 2020 Nov;48(11):1604-1611. doi: 10.1097/CCM.0000000000004554. Crit Care Med. 2020. PMID: 32804785 Free PMC article.
-
Postintubation Dysphagia During COVID-19 Outbreak-Contemporary Review.Dysphagia. 2020 Aug;35(4):549-557. doi: 10.1007/s00455-020-10139-6. Epub 2020 May 28. Dysphagia. 2020. PMID: 32468193 Free PMC article. Review.
-
Clinical application and evaluation of a new type of tracheal catheter fixation belt.Nurs Open. 2023 Apr;10(4):2593-2599. doi: 10.1002/nop2.1519. Epub 2022 Dec 8. Nurs Open. 2023. PMID: 36480230 Free PMC article. Clinical Trial.
-
What Now for Rehabilitation Specialists? Coronavirus Disease 2019 Questions and Answers.Arch Phys Med Rehabil. 2020 Dec;101(12):2233-2242. doi: 10.1016/j.apmr.2020.09.368. Epub 2020 Sep 20. Arch Phys Med Rehabil. 2020. PMID: 32966809 Free PMC article.
-
Laryngeal Injury and Upper Airway Symptoms After Oral Endotracheal Intubation With Mechanical Ventilation During Critical Care: A Systematic Review.Crit Care Med. 2018 Dec;46(12):2010-2017. doi: 10.1097/CCM.0000000000003368. Crit Care Med. 2018. PMID: 30096101 Free PMC article.
References
-
- Wunsch H, Angus DC, Harrison DA, et al. Variation in critical care services across North America and Western Europe. Crit Care Med. 2008;36(10):2787–2793. e2781–2789. - PubMed
-
- Angus DC, Shorr AF, White A, Dremsizov TT, Schmitz RJ, Kelley MA. Critical care delivery in the United States: Distribution of services and compliance with Leapfrog recommendations. Crit Care Med. 2006;34(4):1016–1024. - PubMed
-
- Higgins TL, Kramer AA, Nathanson BH, Copes W, Stark M, Teres D. Prospective validation of the intensive care unit admission Mortality Probability Model (MPM0-III) Crit Care Med. 2009;37(5):1619–1623. - PubMed
-
- Zilberberg MD, de Wit M, Pirone JR, Shorr AF. Growth in adult prolonged acute mechanical ventilation: Implications for healthcare delivery. Crit Care Med. 2008;36(5):1451–1455. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
