

Early Prediction of Intensive Care Unit-Acquired Weakness: A Multicenter External Validation Study
- PMID: 29716425
- PMCID: PMC7222288
- DOI: 10.1177/0885066618771001
Early Prediction of Intensive Care Unit-Acquired Weakness: A Multicenter External Validation Study
Abstract
Objectives: An early diagnosis of intensive care unit-acquired weakness (ICU-AW) is often not possible due to impaired consciousness. To avoid a diagnostic delay, we previously developed a prediction model, based on single-center data from 212 patients (development cohort), to predict ICU-AW at 2 days after ICU admission. The objective of this study was to investigate the external validity of the original prediction model in a new, multicenter cohort and, if necessary, to update the model.
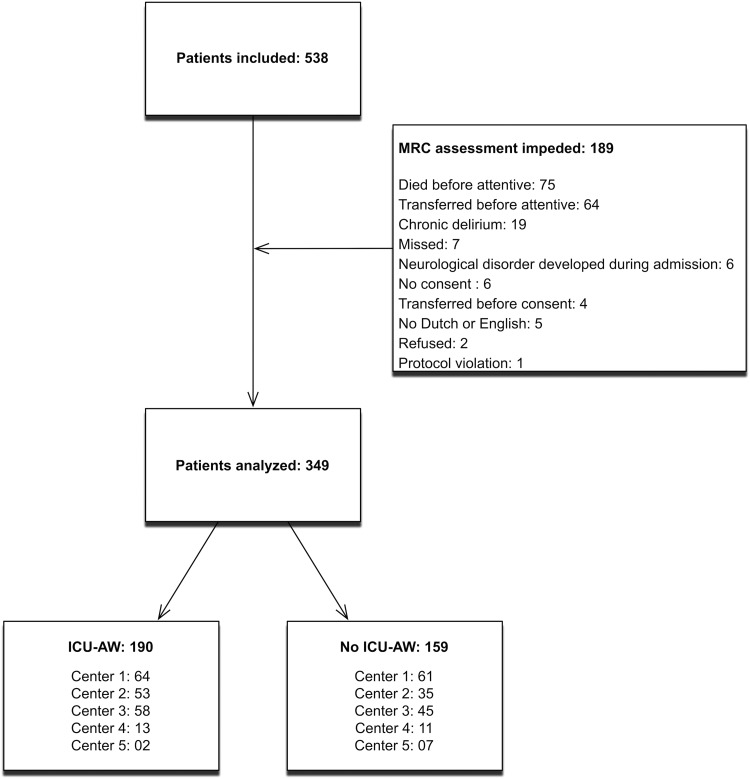
Methods: Newly admitted ICU patients who were mechanically ventilated at 48 hours after ICU admission were included. Predictors were prospectively recorded, and the outcome ICU-AW was defined by an average Medical Research Council score <4. In the validation cohort, consisting of 349 patients, we analyzed performance of the original prediction model by assessment of calibration and discrimination. Additionally, we updated the model in this validation cohort. Finally, we evaluated a new prediction model based on all patients of the development and validation cohort.
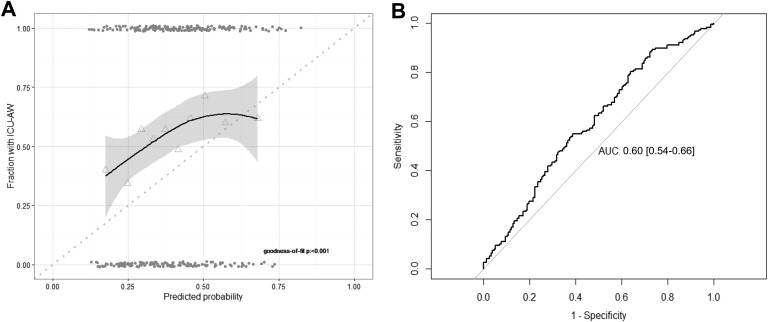
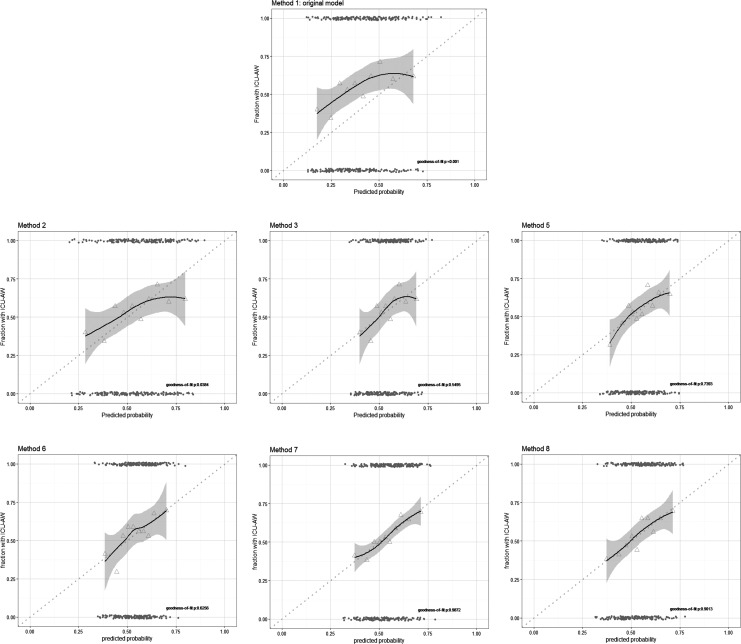
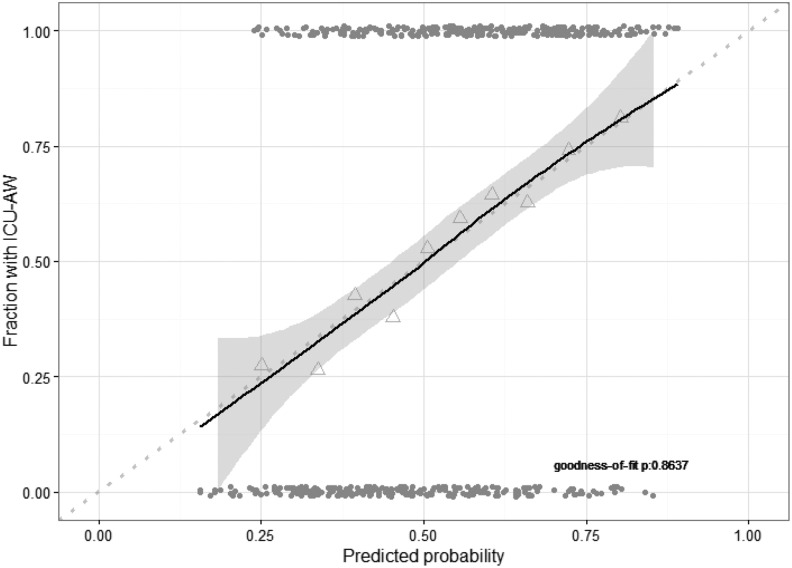
Results: Of 349 analyzed patients in the validation cohort, 190 (54%) developed ICU-AW. Both model calibration and discrimination of the original model were poor in the validation cohort. The area under the receiver operating characteristics curve (AUC-ROC) was 0.60 (95% confidence interval [CI]: 0.54-0.66). Model updating methods improved calibration but not discrimination. The new prediction model, based on all patients of the development and validation cohort (total of 536 patients) had a fair discrimination, AUC-ROC: 0.70 (95% CI: 0.66-0.75).
Conclusions: The previously developed prediction model for ICU-AW showed poor performance in a new independent multicenter validation cohort. Model updating methods improved calibration but not discrimination. The newly derived prediction model showed fair discrimination. This indicates that early prediction of ICU-AW is still challenging and needs further attention.
Keywords: ICU–acquired weakness; external validation; model validation; prediction; prediction model; predictors.
Conflict of interest statement
Figures
References
-
- Stevens RD, Marshall SA, Cornblath DR, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit Care Med. 2009;37(10 suppl):S299–S308. doi:10.1097/CCM.0b013e3181b6ef67. - PubMed
-
- Stevens RD, Dowdy DW, Michaels RK, Mendez-Tellez PA, Pronovost PJ, Needham DM. Neuromuscular dysfunction acquired in critical illness: a systematic review. Inten Care Med. 2007;33(11):1876–1891. - PubMed
-
- Hermans G, Van Mechelen H, Clerckx B, et al. Acute outcomes and 1-year mortality of intensive care unit-acquired weakness. A cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2014;190(4):410–420. doi:10.1164/rccm.201312-2257OC. - PubMed
-
- Tennilä A, Salmi T, Pettilä V, Roine RO, Varpula T, Takkunen O. Early signs of critical illness polyneuropathy in ICU patients with systemic inflammatory response syndrome or sepsis. Inten Care Med. 2000;26(9):1360–1363. doi:10.1007/s001340000586. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
