

Standardised high dose versus low dose cranberry Proanthocyanidin extracts for the prevention of recurrent urinary tract infection in healthy women [PACCANN]: a double blind randomised controlled trial protocol
- PMID: 29716563
- PMCID: PMC5930667
- DOI: 10.1186/s12894-018-0342-7
Standardised high dose versus low dose cranberry Proanthocyanidin extracts for the prevention of recurrent urinary tract infection in healthy women [PACCANN]: a double blind randomised controlled trial protocol
Abstract
Background: Urinary tract infections (UTIs) are amongst the most common bacterial infections affecting women. Although antibiotics are the treatment of choice for UTI, cranberry derived products have been used for many years to prevent UTIs, with limited evidence as to their efficacy. Our objective is to assess the efficacy of a cranberry extract capsule standardized in A-type linkage proanthocyanidins (PACs) for the prevention of recurrent urinary tract infection.
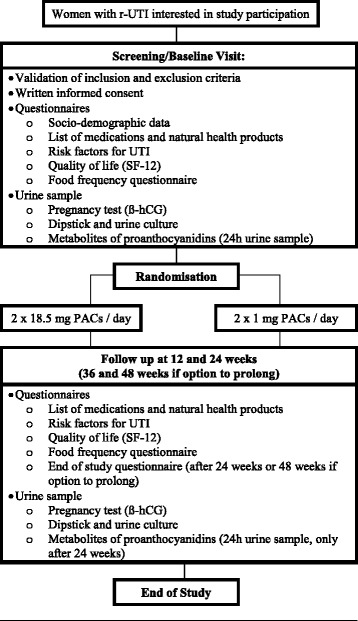
Methods: We will perform a 1:1 randomized, controlled, double blind clinical trial in women aged 18 years or more who present ≥2 UTIs in 6 months or ≥ 3 UTIs in 12 months. One hundred and forty-eight women will be recruited and randomized in two groups to either receive an optimal dose of cranberry extract quantified and standardized in PACs (2 × 18.5 mg PACs per day) or a control dose (2 × 1 mg PACs per day). The primary outcome for the trial is the mean number of new symptomatic UTIs in women during a 6-month intervention period. Secondary outcomes are: (1) To evaluate the mean number of new symptomatic UTIs with pyuria as demonstrated by a positive leucocyte esterase test; (2) To detect the mean number of new symptomatic culture-confirmed UTIs; (3) To quantify urinary PACs metabolites in women who take a daily dose of 37 mg PACs per day compared to women who take a daily dose of 2 mg per day for 6 months; (4) To characterize women who present recurrent UTI based on known risk factors for recurrent UTI; (5) To describe the side effects of daily intake of cranberry extract containing 37 mg PACs compared to 2 mg PACs. This report provides comprehensive methodological data for this randomized controlled trial.
Discussion: The results of this trial will inform urologists, gynaecologists, family physicians and other healthcare professionals caring for healthy women with recurrent UTI, as to the benefits of daily use of an optimal dose of cranberry extract for the prevention of recurrent UTI.
Trial registration: Clinicaltrials.gov, identifier: NCT02572895 October 8th 2015.
Keywords: Antioxidants; Cranberry; Prevention; Proanthocyanidins; Recurrent urinary tract infection; Vaccinium macrocarpon; Women’s health.
Conflict of interest statement
Ethics approval and consent to participate
The protocol and consent form of this study were reviewed and approved by the institutional ethics committee of Laval University with approval number 2015–091 A-5/ 03–11-2016. Further changes to the study protocol will require ethics approval from the institutional ethics committee. The study coordinator will obtain written informed consent from all study participants. Women will be able to withdraw from the study at any time during their participation. Data will be entered electronically and original study forms will be kept locked at the study site and maintained in storage for a period of 25 years after the completion of the study. This randomized clinical trial is registered in
Competing interests
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
