

Coronary microvascular dysfunction in patients with stable coronary artery disease: The CE-MARC 2 coronary physiology sub-study
- PMID: 29716756
- PMCID: PMC6008494
- DOI: 10.1016/j.ijcard.2018.04.061
Coronary microvascular dysfunction in patients with stable coronary artery disease: The CE-MARC 2 coronary physiology sub-study
Abstract
Background: In patients with angina undergoing invasive management, no obstructive coronary artery disease (NOCAD) is a common finding, and angina may persist following percutaneous coronary intervention (PCI). Coronary microvascular dysfunction may be relevant. We aimed to assess the proportion of patients presenting with suspected CAD who had coronary microvascular dysfunction.
Methods: Clinical Evaluation of Magnetic Resonance Imaging in Coronary Heart Disease 2 (CE-MARC 2) was a prospective multicenter randomised controlled trial of functional imaging versus guideline-based management in patients with suspected CAD. Invasive coronary angiography was protocol-directed. Fractional flow reserve (FFR) and parameters of microvascular function (coronary flow reserve (CFR), index of microcirculatory resistance (IMR), resistance reserve ratio (RRR)) were measured in major epicardial coronary arteries with ≥40-≤90% diameter stenosis. An FFR value ≤0.80 indicated the presence of obstructive CAD.
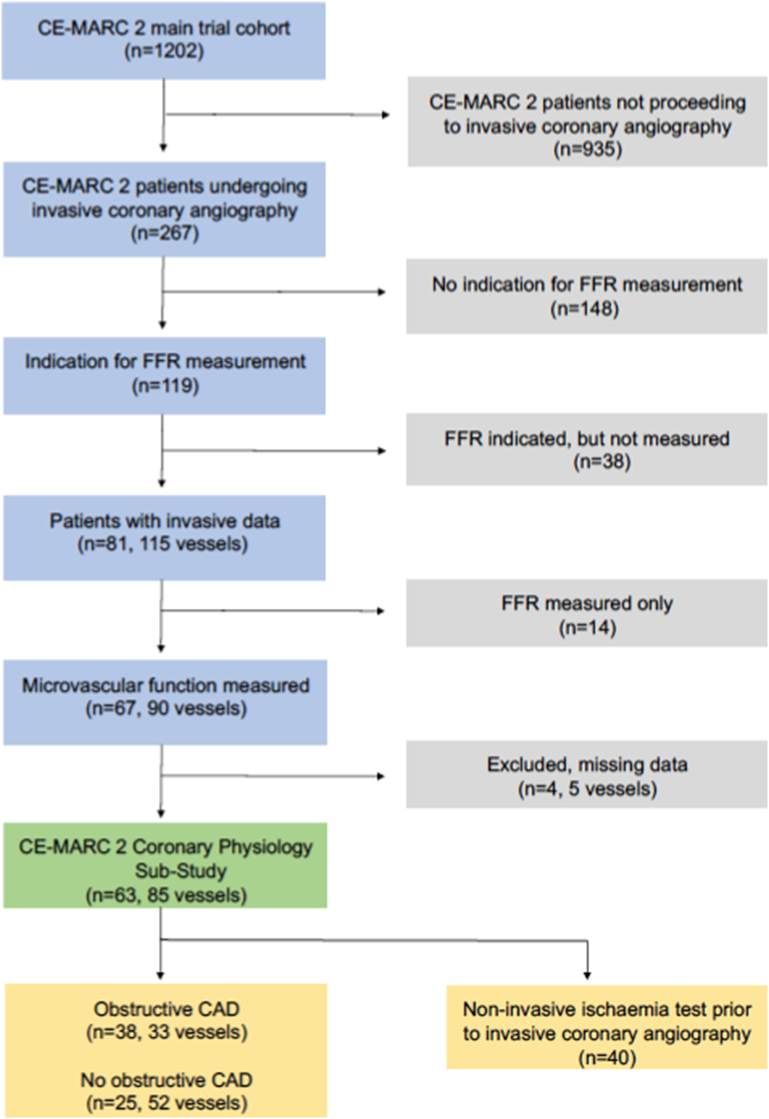
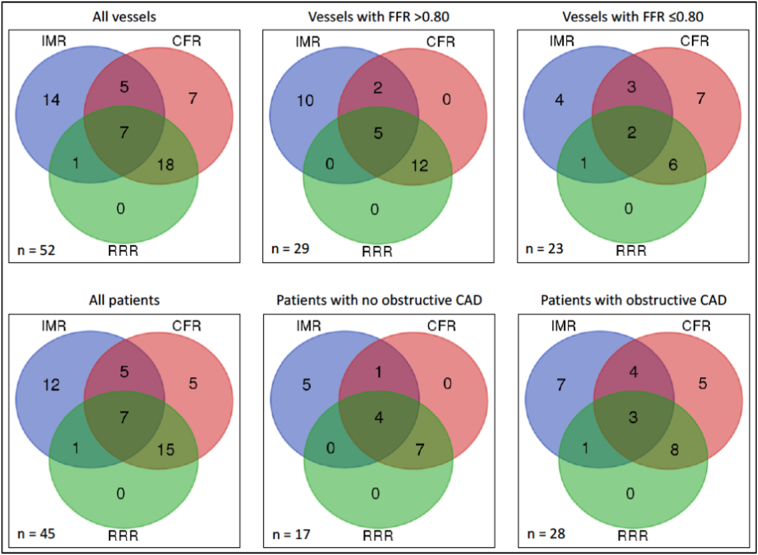
Results: 267/1202 (22.2%) patients underwent angiography and 81 (30%) patients had FFR measured. 63 (78%) of these patients had microvascular function assessed in 85 arteries (mean age 58.5 ± 8.2 years; 47 (75%) male). 25/63 (40%) patients had NOCAD, and of these, 17 (68%) had an abnormality ≥1 parameter of microvascular function (abnormal IMR (≥25), abnormal CFR (<2.0), and abnormal RRR (<2.0) occurred in 10 (40%), 12 (48%), and 11 (44%), respectively). 38/63 (60%) patients had obstructive epicardial CAD. Of these patients, 15/38 (39%), 20/38 (53%), and 12/38 (32%) had an abnormal IMR, CFR and RRR, respectively.
Conclusions: Coronary microvascular dysfunction is common in patients with angina. Invasive assessment of microvascular function may be informative and relevant for decision-making in patients with both NOCAD and obstructive epicardial CAD.
Clinical trial registration: ClinicalTrials.gov Identifier: NCT01664858.
Keywords: Angina; Coronary artery disease; Coronary microvascular dysfunction; Stable ischaemic heart disease.
Copyright © 2018 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Al-Lamee R., Thompson D., Dehbi H.M., Sen S., Tang K., Davies J., Keeble T., Mielewczik M., Kaprielian R., Malik I.S., Nijjer S.S., Petraco R., Cook C., Ahmad Y., Howard J., Baker C., Sharp A., Gerber R., Talwar S., Assomull R., Mayet J., Wensel R., Collier D., Shun-Shin M., Thom S.A., Davies J.E., Francis D.P., investigators O. Percutaneous coronary intervention in stable angina (orbita): A double-blind, randomised controlled trial. Lancet. 2018;391:31–40. - PubMed
-
- Camici P.G., d'Amati G., Rimoldi O. Coronary microvascular dysfunction: mechanisms and functional assessment. Nat. Rev. Cardiol. 2015;12:48–62. - PubMed
-
- Sara J.D., Widmer R.J., Matsuzawa Y., Lennon R.J., Lerman L.O., Lerman A. Prevalence of coronary microvascular dysfunction among patients with chest pain and nonobstructive coronary artery disease. JACC Cardiovasc. Interv. 2015;8:1445–1453. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
