

Robotic resection of Stage III lung cancer: an international retrospective study
- PMID: 29718155
- PMCID: PMC6454562
- DOI: 10.1093/ejcts/ezy166
Robotic resection of Stage III lung cancer: an international retrospective study
Abstract
Objectives: Minimally invasive surgery is accepted for early-stage lung cancer, but its role in locally advanced disease is controversial, especially using a robotic platform. The aim of this retrospective study was to assess the safety and effectiveness of robot-assisted resection in patients with Stage IIIA non-small-cell lung cancer (NSCLC) or carcinoid tumours in the series as a whole and in different subgroups according to adjuvant treatment.
Methods: This was a retrospective multicentre study of consecutive patients with clinically evident or occult N2 disease (210 NSCLC and 13 carcinoid) who, in 2007-2016, underwent robot-assisted resection at 7 high-volume centres. Perioperative outcomes, recurrences and overall survival were assessed.
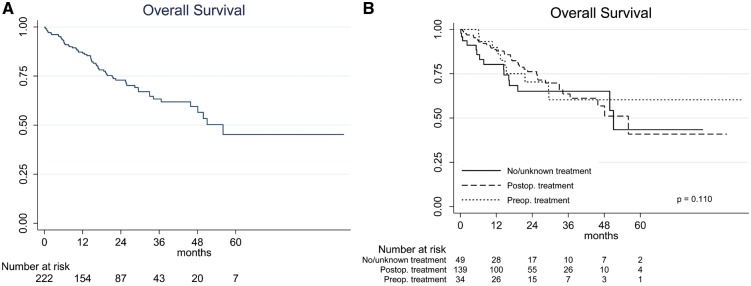
Results: N2 disease was diagnosed preoperatively in 72 (32%) patients and intraoperatively in 151 (68%) patients. Surgical margins were negative in 98.4% of cases with available data. Thirty-four (15.2%) patients received neoadjuvant treatment, 140 (63%) patients received postoperative treatment, and 49 (22%) patients underwent surgery only. There were 22 (9.9%) conversions to thoracotomy, 23 (10.3%) had serious (Grades III-IV) postoperative morbidity and the mean hospital stay was 5.3 days. Complications and outcomes did not differ significantly between treatment groups. Of the 34 patients who were given neoadjuvant chemotherapy, all had R0 resection, 5 (15%) patients required conversion but none required conversion because of bleeding and 4 (12%) patients had Grade III or IV postoperative complications. After a median of 18 (interquartile range 8-33) months, 3-year overall survival in NSCLC patients was 61.2% and 60.3% (P = 0.6) of patients in the subgroup were given induction treatment. However, overall survival was significantly better (P = 0.012) in NSCLC patients with ≤2 positive nodes (vs >2). Nineteen (8.5%) patients developed local recurrence.
Conclusions: Robot-assisted lobectomy is safe and effective in patients with Stage III NSCLC or carcinoid tumours with low conversions and complications. Among patients with NSCLC, including those who were given induction chemotherapy, survival was similar to that reported for open surgery.
Figures

Comment in
-
Robotic resection of stage III lung cancer: an international retrospective study.J Thorac Dis. 2018 Sep;10(Suppl 26):S3081-S3083. doi: 10.21037/jtd.2018.07.90. J Thorac Dis. 2018. PMID: 30370084 Free PMC article. No abstract available.
References
-
- Demmy TL, Curtis JJ.. Minimally invasive lobectomy directed toward frail and high-risk patients a case-control study. Ann Thorac Surg 1999;68:194–200. - PubMed
-
- Hoksch B, Ablassmaier B, Walter M, Muller JM.. Complication rate after thoracoscopic and conventional lobectomy. Zentralblatt Fur Chirurgie 2003;128:106–10. - PubMed
-
- Nakata M, Saeki H, Yokoyama N, Kurita A, Takiyama W, Takashima S.. Pulmonary function after lobectomy video-assisted thoracic surgery versus thoracotomy. Ann Thorac Surg 2000;70:938–41. - PubMed
-
- Nomori H, Ohtsuka T, Horio H, Naruke T, Suemasu K.. Difference in the impairment of vital capacity and 6-minute walking after a lobectomy performed by thoracoscopic surgery, an anterior limited thoracotomy, an anteroaxillary thoracotomy, and a posterolateral thoracotomy. Surg Today 2003;33:7–12. - PubMed
-
- Yim AP, Wan S, Lee TW, Arifi AA.. VATS lobectomy reduces cytokine responses compared with conventional surgery. Ann Thorac Surg 2000;70:243–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
