

Association of plexiform neurofibroma volume changes and development of clinical morbidities in neurofibromatosis 1
- PMID: 29718344
- PMCID: PMC6231202
- DOI: 10.1093/neuonc/noy067
Association of plexiform neurofibroma volume changes and development of clinical morbidities in neurofibromatosis 1
Abstract
Background: Plexiform neurofibromas (PN) in neurofibromatosis 1 (NF1) can cause substantial morbidities. Clinical trials targeting PN have recently described decreases in PN volumes. However, no previous study has assessed the association between changes in PN volumes and PN-related morbidities. Our objective was to assess if increasing PN volume in NF1 is associated with increasing PN-related morbidity.
Methods: This is a retrospective review of patients enrolled on the NCI NF1 natural history study with ≥7 years of data available. Morbidities including pain, motor dysfunction, vision loss, and PN-related surgery were assessed at time of baseline PN MRI with volumetric analysis and time of MRI with maximum PN volume.
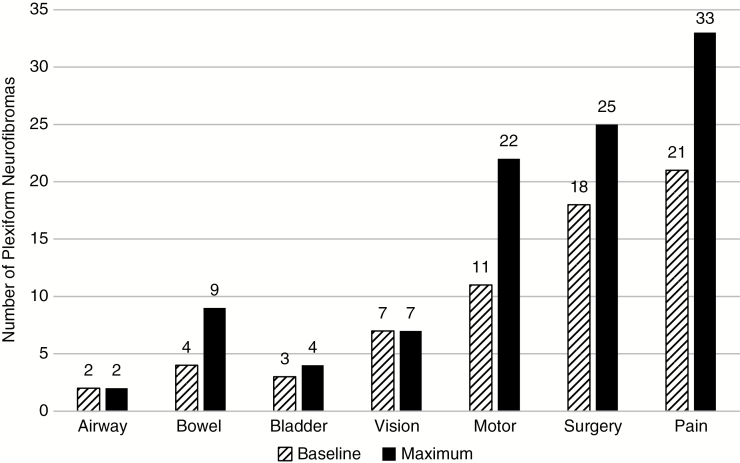
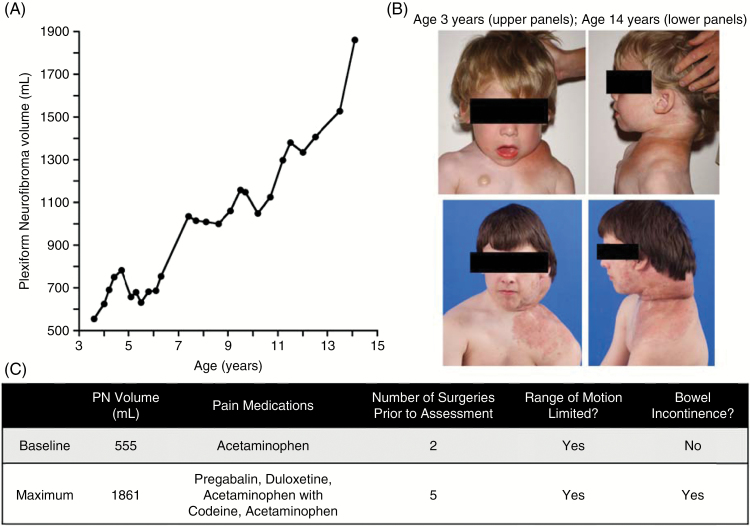
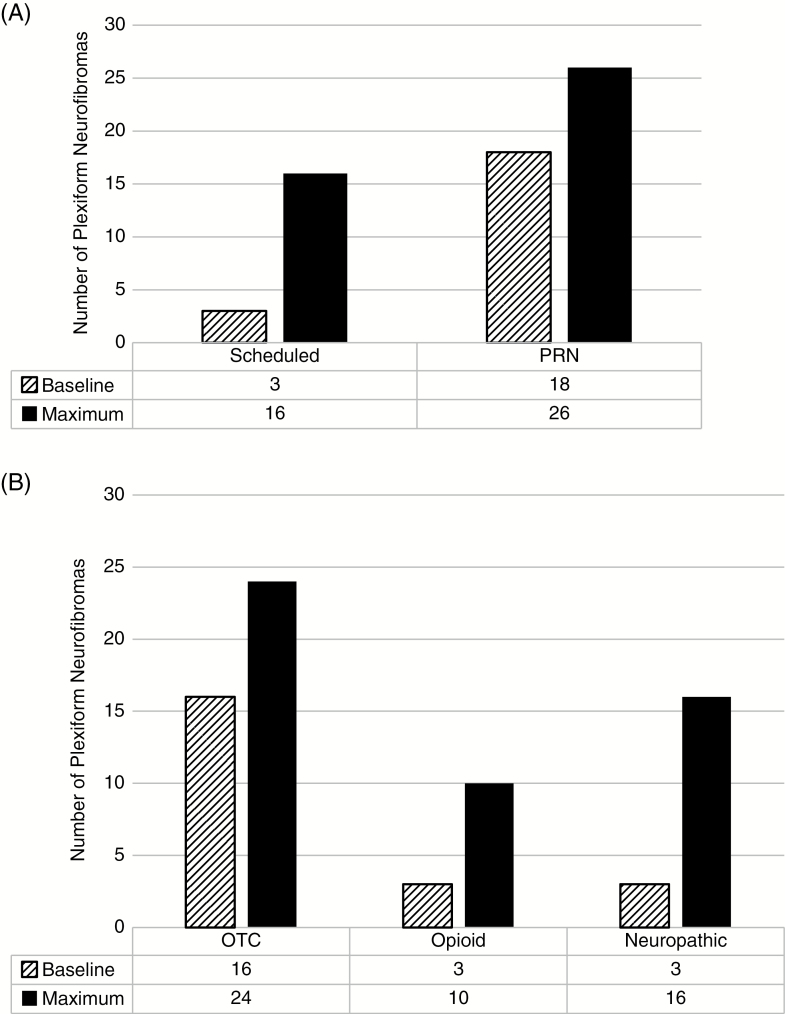
Results: Forty-one patients (median age at baseline 8 y) with 57 PN were included. At baseline, 40 PN had at least 1 PN-associated morbidity. During the observation period, 27 PN required increasing pain medication, and these PN grew faster per year (median difference 8.3%; 95% CI: 2.4, 13.8%) than those PN which did not. PN resulting in motor impairment at baseline (n = 11) had larger volumes compared with those that did not (median difference 461 mL; 95% CI: 66.9, 820).
Conclusions: Many NF1 PN were associated with clinically significant morbidity at baseline, highlighting the need for longitudinal morbidity evaluations starting at an early age to capture changes in PN-associated morbidities. Prospective evaluation of standardized patient reported and functional outcomes in clinical trials are ongoing and may allow further characterization of the association of PN volume increase or decrease and clinical changes.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
